

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 13, Number 6, December 2022, pages 333-338

Percutaneous Coronary Intervention Outcomes in Patients With Prior Thoracic Radiation Therapy: A Systematic Review and Meta-Analysis
Ravi Thakkera, f, Krishna Sutharb, Pooja Bhaktac, Marissa Leec, Deaa Abu Jazarc, Milee Patelc, Ayman Elbadawid, Aiham Albaenia, Syed Mustajab Hasana, Mohammed Faluka, Maurice Willise, Khaled Chatilaa, Wissam Khalifea, Umamahesh Rangasettya, Afaq Motiwalaa, Syed Gilania, Hani Jneida
aDivision of Cardiology, University of Texas Medical Branch, Galveston, TX, USA
bDivision of Hematology and Oncology, Baylor Scott and White Medical Center, Temple, TX, USA
cDepartment of Internal Medicine, University of Texas Medical Branch, Galveston, TX, USA
dDivision of Cardiology, University of Texas Southwestern Medical Center, Dallas, TX, USA
eDepartment of General Oncology, MD Anderson Cancer Center, Galveston, TX, USA
fCorresponding Author: Ravi Thakker, Division of Cardiology, University of Texas Medical Branch, Galveston, TX 77555, USA
Manuscript submitted August 20, 2022, accepted September 19, 2022, published online November 14, 2022
Short title: PCI Outcomes in Prior Thoracic Radiation
doi: https://doi.org/10.14740/cr1426
| Abstract | ▴Top |
Background: Thoracic radiation predisposes patients to accelerated coronary artery disease. There is a paucity of data in both short-term and long-term outcomes following revascularization in patients who have undergone thoracic radiation.
Methods: We performed a search of the Medline, Cochrane, and Scopus databases for studies that compared outcomes in cancer patients who have undergone thoracic radiation and percutaneous coronary intervention (PCI). The primary outcome of our meta-analysis was all-cause mortality. Secondary outcomes included cardiac mortality, myocardial infarction (MI), and restenosis.
Results: The analysis included four observational studies with a total of 13,941 patients for the primary outcome of all-cause mortality. There were a total of 1,322 patients analyzed for cardiac mortality, 13,103 for MI, and 10,530 for restenosis. The longest follow-up for the primary outcome was 16 years. There was statistically significant higher risk of all-cause mortality in patients who underwent thoracic radiation (risk ratio (RR): 1.29, 95% confidence interval (CI): 1.08 - 1.54, P = 0.004). There was no statistically significant difference in cardiac mortality (RR: 1.15, 95% CI: 0.83 - 1.61, P = 0.40), MI (RR: 1.01, 95% CI: 0.20 - 5.08, P = 0.99), and restenosis (RR: 1.92, 95% CI: 0.24 - 15.35, P = 0.54).
Conclusion: In this meta-analysis, we found a higher risk of all-cause mortality in patients with a history of thoracic radiation undergoing PCI, likely from underlying malignancy itself.
Keywords: Cardiotoxicity; Coronary restenosis; Coronary artery disease; Radiation
| Introduction | ▴Top |
Over the past several years, life expectancy in patients with malignancies has improved as a result of novel treatment approaches. Radiation therapy has become a hallmark of this longevity and accounts for treatment in approximately half of all malignancies, notably Hodgkin’s lymphoma and breast cancer [1]. Coronary artery disease (CAD) in patients who have undergone radiation therapy is a well-known complication, with a prevalence of up to 85%. In terms of revascularization, there is no consensus, and most patients are treated similarly to their non-irradiated counterparts, with percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG) [2]. Given the paucity in data, we performed a systematic review and meta-analysis evaluating outcomes in patients who have undergone thoracic radiation and underwent PCI.
| Materials and Methods | ▴Top |
Data sources and search strategy
A search of the MEDLINE, Cochrane, and Scopus databases was performed from inception until March 2022 using the following search terms: “percutaneous coronary intervention”, “coronary artery disease”, “percutaneous coronary revascularization”, “mediastinal radiation”, “thoracic radiation” in combination or separately to identify articles evaluating outcomes in cancer patients who have undergone thoracic radiation and PCI. No language restrictions were applied. This meta-analysis was performed following the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines (Supplementary Material 1, www.cardiologyres.org) [3]. IRB approval is not applicable as it is a meta-analysis. This study was conducted in compliance with the ethical standards of the responsible institution on human subjects as well as with the Helsinki Declaration.
Inclusion and exclusion criteria
Inclusion criteria included studies that evaluated outcomes in cancer patients who had undergone thoracic radiation with cardiac involvement and PCI that additionally included a control group of CAD requiring PCI without thoracic radiation. Patients who had undergone mediastinal radiation were additionally included. Case reports, case series, and case control studies were excluded due to inherently higher risk of bias and difficulty assessing validity in these studies. Studies were also excluded if they did not have a control group or compared outcomes between PCI and CABG patients.
Data extraction
Final studies for inclusion in the analysis were obtained by authors RT, PB, ML, and DAJ. Data were extracted by authors RT and MP. Data were verified by authors RT, PB, and MP. If discrepancies occurred, they were resolved through joint discussion among all authors.
Outcomes
The primary outcome of this study was all-cause mortality in cancer patients undergoing thoracic radiation and PCI. Secondary outcomes included cardiac mortality, myocardial infarction (MI), and coronary stent restenosis.
Evaluation of quality of included studies
Bias was assessed using the Newcastle-Ottawa Scale as seen in Supplementary Material 2 (www.cardiologyres.org) [4].
Statistical analysis
Due to the potential for heterogeneity among the studies identified for our analysis, a random-effects model was utilized. The effect measure for our variables was relative risk (RR). P-values were statistically significant if < 0.05. Heterogeneity was obtained using I2 statistics [5]. Analysis was conducted with the RevMan 5.4 software (Cochrane Collaboration, Oxford, UK).
| Results | ▴Top |
Our meta-analysis identified four observational studies with a total of 13,941 patients who had undergone thoracic radiation and PCI for our primary outcome of all-cause mortality [6-9]. The study selection according to PRISMA criteria can be found in Figure 1. Baseline characteristics of the patient population in the four studies can be found in Tables 1 and 2.
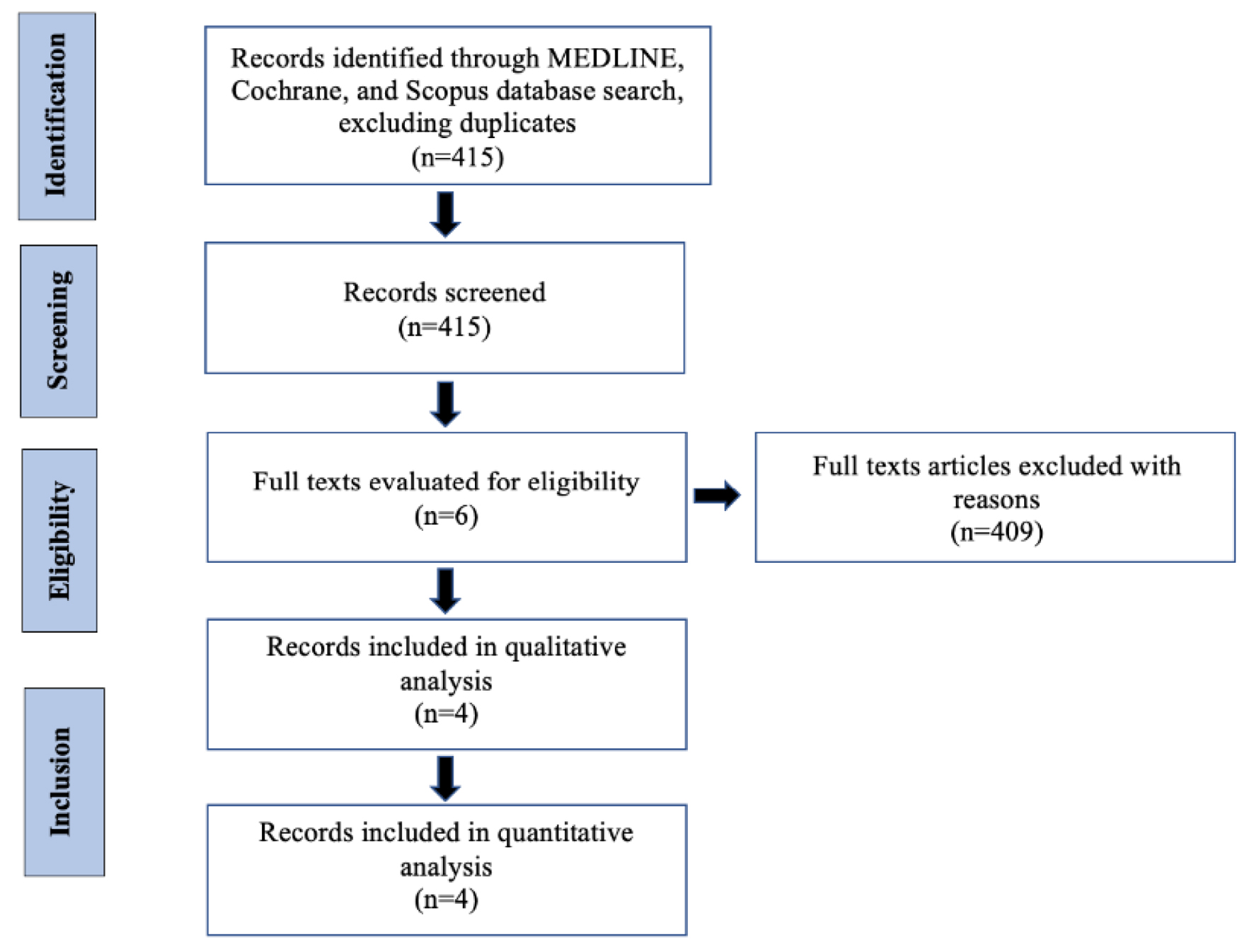 Click for large image | Figure 1. PRISMA study flow sheet. |
 Click to view | Table 1. Patient Baseline Characteristics |
Click to view | Table 2. Angiographic Characteristics |
Primary and secondary outcomes
The primary outcome of this study was all-cause mortality derived from all four studies [6-9]. All-cause mortality after PCI was significantly higher in patients with a history of thoracic radiation compared to those with no history of prior thoracic radiation (risk ratio (RR): 1.29, 95% confidence interval (CI): 1.08 - 1.54, P = 0.004, I2 = 0%) (Fig. 2). There were a total of 1,322 patients analyzed for cardiac mortality among three studies [7-9], and 13,103 for MI and 10,530 for restenosis among two studies [6, 7]. There was a numerically increased risk of cardiac mortality (RR: 1.15, 95% CI: 0.83 - 1.61, P = 0.40, I2 = 0%) (Fig. 3), MI (RR: 1.01, 95% CI: 0.20 - 5.08, P = 0.99, I2 = 48%) (Fig. 4), and restenosis (RR: 1.92, 95% CI: 0.24 - 15.35, P = 0.54) (Fig. 5) in the radiation group but it did not reach statistical significance. There was significant heterogeneity in Pheterogeneity < 0.0001, I2 = 94% in the restenosis group.
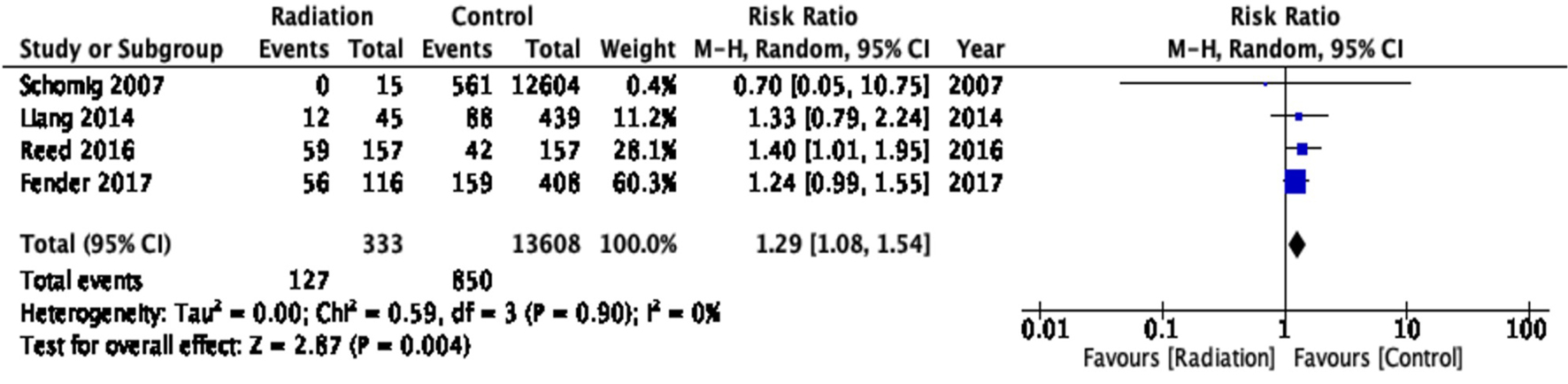 Click for large image | Figure 2. All-cause mortality. |
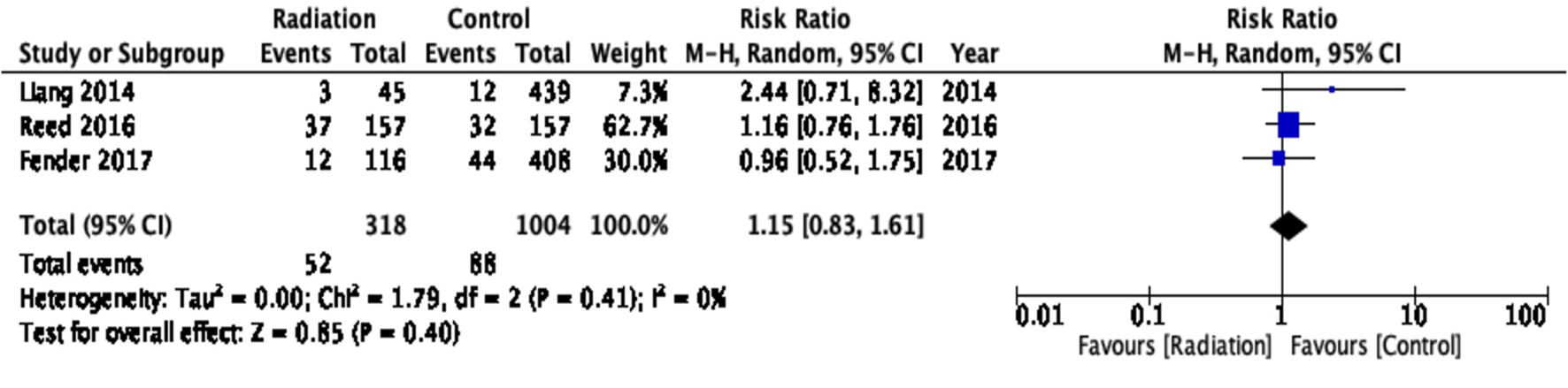 Click for large image | Figure 3. Cardiac mortality. |
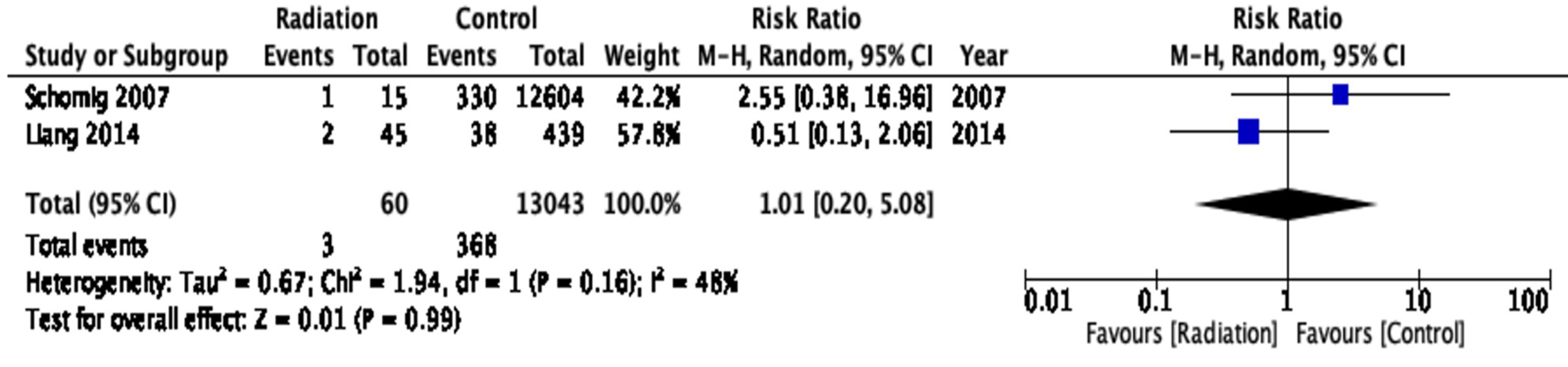 Click for large image | Figure 4. Myocardial infarction. |
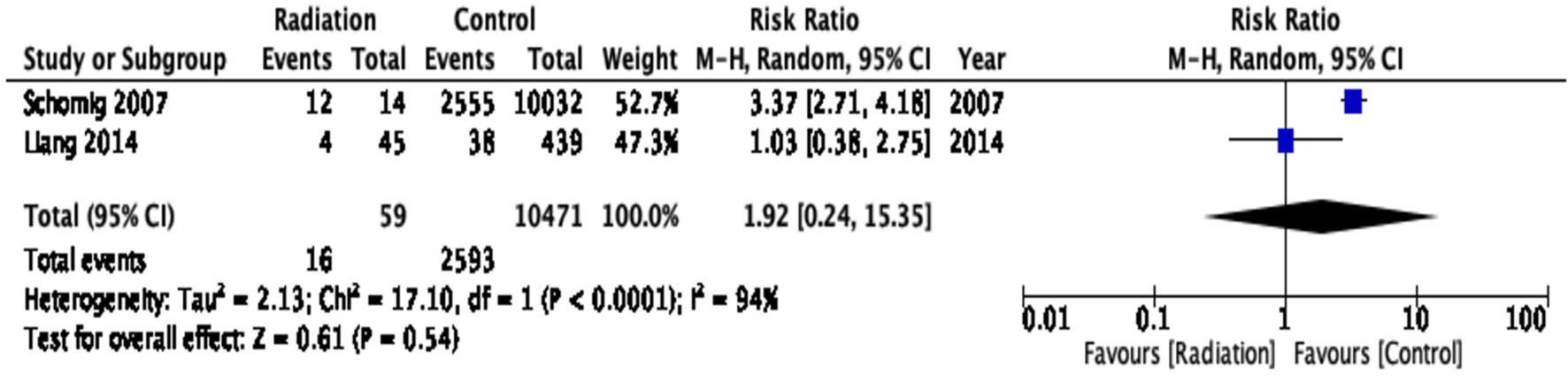 Click for large image | Figure 5. Restenosis. |
| Discussion | ▴Top |
In our analysis of 13,941 patients from four observational studies looking at post-PCI outcomes with and without a history of prior thoracic radiation, we found that there is a higher risk of all-cause mortality among patients who underwent thoracic radiation and PCI. Furthermore, there was no statistically significant risk in cardiac mortality, MI, or restenosis when compared to patients who did not receive prior thoracic radiation.
Numerous studies have shown an increased risk of premature cardiovascular disease in cancer survivors with prior radiation exposure [10]. Radiation leading to arteriosclerosis has been a known phenomenon for decades [11]. The American Society of Echocardiography recommends screening patients for radiation-induced heart disease with imaging modalities such as transthoracic echocardiogram, cardiac magnetic resonance, or coronary computed tomography angiography in those who have received more than 35 Gy of radiation [10]. The timing recommended for screening is either 5 years after completion of radiation therapy or after ages 30 to 35 years. Equally important, evaluation should be done in patients who develop any new cardiac symptoms. Risk factors for developing radiation-induced CAD include hypercholesterolemia, diabetes mellitus, chronic obstructive pulmonary disease, smoking history, and elevated body mass index [12]. Prevention is focused on limiting radiation delivered through a multimodality approach such as intensity-modulated radiation therapy, breath holding, image-guided radiation therapy, and four-dimensional imaging. Management of CAD in such patients is often complex, with limited data to guide treatment decisions. Surgery has been reported to have higher rates of complications including mortality due to radiation-related changes in anatomy such as scar tissues or even adhesions around the heart, pericardium, lung or other organs [13].
Radiation-induced CAD was first described in 1957 [14]. In patients receiving radiation for breast cancer, the risk for radiation-induced coronary injury increases within the first 5 years after exposure and continues for at least 20 years [15]. This risk is even higher in patients receiving radiation therapy for lymphoma due to higher radiation doses [16]. The exact mechanism of radiation-induced CAD is still being investigated. The major pathways are believed to be endothelial cell death and changes in endothelial cell environment. In terms of endothelial cell death, it is believed that DNA damage secondary to ionizing radiation results in cell cycle arrest and ultimately endothelial senescence and apoptosis. Through the endothelial senescence, there is activation of inflammatory markers that results in oxidative changes and low-density lipoprotein (LDL) deposition in the vascular endothelium. The apoptosis pathway leads to accelerated atherosclerosis. In terms of the cell environment, the mechanisms purported to play a role include changes in cell adhesion structure, increased coagulopathy, increased reactive oxygen species, inflammatory cytokines, angiogenesis, glycolysis, and immune system activation [17].
Our analysis of four observational studies revealed a higher risk of all-cause mortality in patients with previous radiation therapy who underwent PCI. Upon closer examination of the individual studies [6-9], we noted discrepant findings with regards to all-cause mortality. Three studies did not show increased mortality in patients who underwent radiation and PCI [6, 7, 9], while the remaining one study did show an increase in mortality [8]. In terms of cardiac mortality, our findings were similar to those of Liang et al and Fender et al [7, 9], who did not demonstrate statistical significance, but contrasted the findings of Reed et al [8]. Our findings of non-significance in stent restenosis were similar to Liang et al [7] but contrasted those of Schomig et al [6]. The high degree of heterogeneity when evaluating restenosis can likely be explained by the limited number of studies, as well as difference in end points with 6-month evaluation by Schomig et al [6] and 3 years by Liang et al [7].
There are limitations to our analysis. The number of studies evaluating our outcomes was limited, although there was a decent population size. There was a large difference in population size among the control and events group in the study by Schomig et al [6]. Although, we aimed to reduce heterogeneity with a random-effects model. There was a high degree of heterogeneity when evaluating restenosis likely secondary to only two studies being analyzed. Schomig et al [6] had a large difference in population between the control and treatment group. The study also was completed prior to drug-eluting stents in the late 1990s and early 2000s [18]. Furthermore, Schomig et al evaluated restenosis at 6 months [6], while Liang et al’s longest follow-up was at 3 years [7].
Conclusion
In our meta-analysis of a small number of studies examining post-PCI outcomes in cancer patients, we found a statistically significant higher risk of all-cause mortality post-PCI in patients with a history of prior thoracic radiation therapy compared to those with no prior thoracic radiation, likely, attributably to malignancy itself. Additionally, we found no statistically significant increase in risk of cardiac mortality, MI, or restenosis in patients with prior thoracic radiation therapy compared to those without prior thoracic radiation. Further large-scale studies are needed to better appreciate both short-term and long-term outcomes in patients who undergo thoracic radiation therapy and PCI.
| Supplementary Material | ▴Top |
Suppl 1. PRISMA guidelines.
Suppl 2. Newcastle-Ottawa scale.
Acknowledgments
None to declare.
Financial Disclosure
The authors have no financial disclosure to declare.
Conflict of Interest
The authors have no conflict of interest to declare.
Informed Consent
Not applicable.
Author Contributions
Study conception and design: RT. Manuscript preparation/drafting: RT, KS, PB, ML, DAJ, MP, AE, AA, SMH, and MF. Expert review: MW, KC, WK, UR, AM, SG, and HJ.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
CAD, coronary artery disease; PCI, percutaneous coronary intervention; MI, myocardial infarction; PRISMA, Preferred Reporting Items for Systematic Review and Meta-Analysis; CABG, coronary artery bypass grafting; MVD, multivessel disease; LAD, left anterior descending artery; RR, risk ratio; CI, confidence interval
| References | ▴Top |
- Raghunathan D, Khilji MI, Hassan SA, Yusuf SW. Radiation-induced cardiovascular disease. Curr Atheroscler Rep. 2017;19(5):22.
doi pubmed - Jaworski C, Mariani JA, Wheeler G, Kaye DM. Cardiac complications of thoracic irradiation. J Am Coll Cardiol. 2013;61(23):2319-2328.
doi pubmed - Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
doi pubmed - Hartling L, Hamm M, Milne A, Vandermeer B, Santaguida PL, Ansari M, Tsertsvadze A, et al.: In: Validity and inter-rater reliability testing of quality assessment instruments. Rockville (MD), 2012.
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557-560.
doi pubmed - Schomig K, Ndrepepa G, Mehilli J, Pache J, Kastrati A, Schomig A. Thoracic radiotherapy in patients with lymphoma and restenosis after coronary stent placement. Catheter Cardiovasc Interv. 2007;70(3):359-365.
doi pubmed - Liang JJ, Sio TT, Slusser JP, Lennon RJ, Miller RC, Sandhu G, Prasad A. Outcomes after percutaneous coronary intervention with stents in patients treated with thoracic external beam radiation for cancer. JACC Cardiovasc Interv. 2014;7(12):1412-1420.
doi pubmed - Reed GW, Masri A, Griffin BP, Kapadia SR, Ellis SG, Desai MY. Long-term mortality in patients with radiation-associated coronary artery disease treated with percutaneous coronary intervention. Circ Cardiovasc Interv. 2016;9(6):e003483.
doi pubmed - Fender EA, Liang JJ, Sio TT, Stulak JM, Lennon RJ, Slusser JP, Ashman JB, et al. Percutaneous revascularization in patients treated with thoracic radiation for cancer. Am Heart J. 2017;187:98-103.
doi pubmed - Belzile-Dugas E, Eisenberg MJ. Radiation-induced cardiovascular disease: review of an underrecognized pathology. J Am Heart Assoc. 2021;10(18):e021686.
doi pubmed - Annest LS, Anderson RP, Li W, Hafermann MD. Coronary artery disease following mediastinal radiation therapy. J Thorac Cardiovasc Surg. 1983;85(2):257-263.
doi - Groarke JD, Nguyen PL, Nohria A, Ferrari R, Cheng S, Moslehi J. Cardiovascular complications of radiation therapy for thoracic malignancies: the role for non-invasive imaging for detection of cardiovascular disease. Eur Heart J. 2014;35(10):612-623.
doi pubmed - Yang EH, Marmagkiolis K, Balanescu DV, Hakeem A, Donisan T, Finch W, Virmani R, et al. Radiation-induced vascular disease-a state-of-the-art review. Front Cardiovasc Med. 2021;8:652761.
doi pubmed - Gustavsson A, Eskilsson J, Landberg T, Svahn-Tapper G, White T, Wollmer P, Akerman M. Late cardiac effects after mantle radiotherapy in patients with Hodgkin's disease. Ann Oncol. 1990;1(5):355-363.
doi pubmed - Darby SC, Ewertz M, McGale P, Bennet AM, Blom-Goldman U, Bronnum D, Correa C, et al. Risk of ischemic heart disease in women after radiotherapy for breast cancer. N Engl J Med. 2013;368(11):987-998.
doi pubmed - van Leeuwen-Segarceanu EM, Bos WJ, Dorresteijn LD, Rensing BJ, der Heyden JA, Vogels OJ, Biesma DH. Screening Hodgkin lymphoma survivors for radiotherapy induced cardiovascular disease. Cancer Treat Rev. 2011;37(5):391-403.
doi pubmed - Venkatesulu BP, Mahadevan LS, Aliru ML, Yang X, Bodd MH, Singh PK, Yusuf SW, et al. Radiation-induced endothelial vascular injury: a review of possible mechanisms. JACC Basic Transl Sci. 2018;3(4):563-572.
doi pubmed - Iqbal J, Gunn J, Serruys PW. Coronary stents: historical development, current status and future directions. Br Med Bull. 2013;106:193-211.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.