

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website http://www.cardiologyres.org |
Case Report
Volume 9, Number 3, June 2018, pages 171-172
Rotablation for Stent Underexpansion: An Effective Alternative
Michael Spartalisa, b, f, Diamantis I. Tsilimigrasc, Demetrios Morisd, Christos Kontogiannise, Dimitrios C. Iliopoulosc, Eleftherios Spartalisc
aDivision of Cardiology, Onassis Cardiac Surgery Center, Athens, Greece
bESC Working Group on Thrombosis, Sophia Antipolis, France
cLaboratory of Experimental Surgery and Surgical Research, University of Athens Medical School, Athens, Greece
dDepartment of Surgery, Duke University, Durham, NC, USA
eDepartment of Clinical Therapeutics, "Alexandra" Hospital, University of Athens, Athens, Greece
fCorresponding Author: Michael Spartalis, 356 Syggrou Ave, Athens 176 74, Greece
Manuscript submitted December 25, 2017, accepted January 29, 2018
Short title: Rotablation for Stent Underexpansion
doi: https://doi.org/10.14740/cr670w
| Abstract | ▴Top |
A 75-year old female was evaluated for recurrent angina. She had an underexpanded stent. Conventional methods failed to achieve a full stent expansion. Rotablation resulted in an excellent angiographic outcome and full stent deployment. The patient remains angina-free at 1-year follow-up.
Keywords: Rotablation; Angiography; Stent underexpansion; Restenosis; Angioplasty
| Introduction | ▴Top |
Rotational atherectomy (RA) is a technique currently used as a different strategy for treating heavily calcified lesions during percutaneous coronary intervention (PCI), in order to facilitate optimal stent delivery and expansion [1]. RA has evolved from plaque debulking technique to plaque modification [1]. The current management of plaque modification followed by stent implantation has remarkedly reduced the incidence of acute complications, but the efficacy of this method is highly operator dependent [1].
| Case Report | ▴Top |
A 75-year old female with a history of an anterior myocardial infarction, treated with direct culprit vessel primary percutaneous coronary intervention (PCI) of left anterior descending (LAD) artery, presented with recurrent angina Canadian Cardiovascular Society class III. Stress echocardiography revealed decreased coronary flow reserve in the LAD territory. Coronary angiography showed a mid-LAD 99% in-stent restenosis (ISR) due to stent underdeployment and an intraluminal filling defect (thrombus) (Fig. 1a). Rotablation atherectomy with 1.5 mm burr was attempted, and the ablation was initiated at the proximal edge of the stent. After 12 runs of rotational atherectomy using speeds of 200,000 rpm, a 3.0 × 8 mm balloon was inflated to 16 atm within the stent, with evidence of full balloon and stent expansion, resulting in an excellent angiographic result (TIMI flow III) (Fig. 1b). At 1-year follow-up, the patient is asymptomatic.
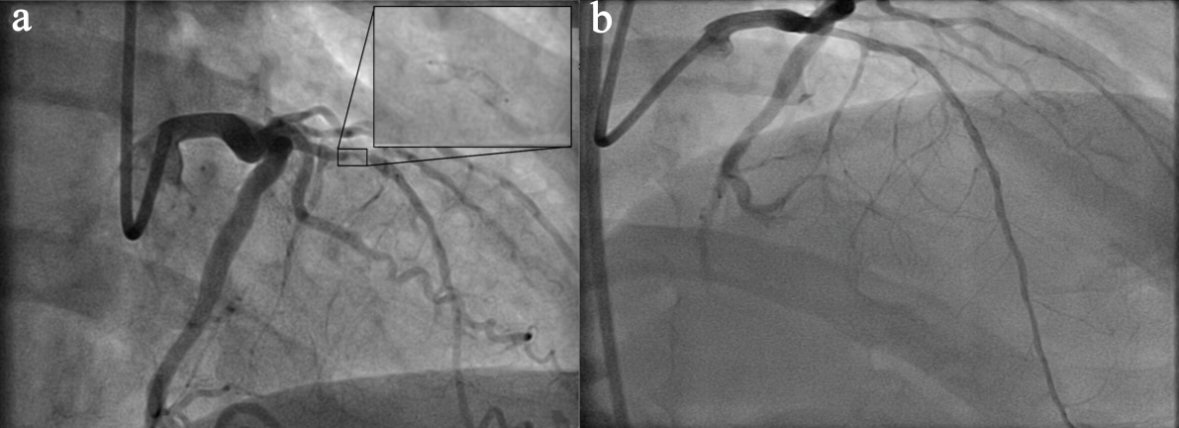 Click for large image | Figure 1. (a) Coronary angiography showing a mid-LAD 99% in-stent restenosis, an angiographic image suggestive of intra-stent thrombus. (b) Coronary angiography after rotational atherectomy showing a fully expanded LAD stent with TIMI III flow. |
| Discussion | ▴Top |
Drug-eluting stents (DES) have decreased the possibility of ISR. The current rate of ISR in the DES era remains higher than 10% [1]. RA in combination with DES implantation is an effective alternative approach in treating ISR [1]. The role of RA, as a treatment option for heavily calcified lesions, is well established in the literature [1-3]. Our case illustrates the clinical significance of RA in treating stent underexpansion in non-calcified lesions. Rotablation induces thermal injury and heat generation, causing the metal to erode and allowing balloon dilation and full expansion. This technique can be used when conventional methods are unsuccessful. We propose to broaden the use of rotablation in stent underexpansion, as has proven to be a safe and effective alternative [1-3].
Conflict of Interest
All authors have contributed and approved the final version of this manuscript. No author has any conflict of interest to disclose.
Financial Support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
| References | ▴Top |
- Barbato E, Shlofmitz E, Milkas A, Shlofmitz R, Azzalini L, Colombo A. State of the art: evolving concepts in the treatment of heavily calcified and undilatable coronary stenoses - from debulking to plaque modification, a 40-year-long journey. EuroIntervention. 2017;13(6):696-705.
doi pubmed - Stankovic G, Milasinovic D. Rotational atherectomy in clinical practice: the art of tightrope walking. Circ Cardiovasc Interv. 2016;9(11):e004571.
doi pubmed - Sakakura K, Inohara T, Kohsaka S, Amano T, Uemura S, Ishii H, Kadota K, et al. Incidence and determinants of complications in rotational atherectomy: insights from the national clinical data (J-PCI Registry). Circ Cardiovasc Interv. 2016;9(11):e004278.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.