

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Review
Volume 14, Number 1, February 2023, pages 12-21

Glucagon-Like Peptide 1 Receptor Agonists Versus Sodium-Glucose Cotransporter 2 Inhibitors for Atherosclerotic Cardiovascular Disease in Patients With Type 2 Diabetes
Hidekatsu Yanaia, b, Hiroki Adachia, Mariko Hakoshimaa, Hisayuki Katsuyamaa
aDepartment of Diabetes, Endocrinology and Metabolism, National Center for Global Health and Medicine Kohnodai Hospital, Chiba, Japan
bCorresponding Author: Hidekatsu Yanai, Department of Diabetes, Endocrinology and Metabolism, National Center for Global Health and Medicine Kohnodai Hospital, 1-7-1 Kohnodai, Ichikawa, Chiba 272-8516, Japan
Manuscript submitted December 26, 2022, accepted February 11, 2023, published online February 25, 2023
Short title: GLP-1RA vs. SGLT2i for ASCVD
doi: https://doi.org/10.14740/cr1459
- Abstract
- Introduction
- The Association Between Risk Reduction of MACE and Changes in ASCVD Risk Factors
- Effects of GLP-1RA and SGLT2i on the Surrogate Marker for Atherosclerosis
- Effects of GLP-1RA and SGLT2i on ASCVD Risk Factors
- Vascular Biological Anti-Atherogenic Properties of GLP-1RA
- Conclusion
- References
| Abstract | ▴Top |
Beyond improving hemoglobin A1c (HbA1c) in adults with type 2 diabetes, glucagon-like peptide 1 receptor agonists (GLP-1RA) have been approved for reducing risk of major adverse cardiovascular events (MACE) with established cardiovascular disease (CVD) or multiple CV risk factors. Sodium-glucose cotransporter 2 inhibitors (SGLT2i) also reduced the risk for the primary composite CV outcome in patients with type 2 diabetes at high risk for CV events. In the American Diabetes Association (ADA) and European Association of Study in Diabetes (EASD) consensus report 2022, there is the description “In people with established atherosclerotic CVD (ASCVD) or with a high risk for ASCVD, GLP-1RA were prioritized over SGLT2i”; however, the evidence supporting such statement is limited. Therefore, we studied the superiority of GLP-1RA over SGLT2i for prevention of ASCVD from various viewpoints. We could not find a meaningful difference in the risk reduction in three-point MACE (3P-MACE), mortality due to any cause, mortality due to CV cause and nonfatal myocardial infarction between GLP-1RA and SGLT2i trials. The risk of nonfatal stroke decreased in all five GLP-1RA trials; however, two of three SGLT2i trials showed an increase in risk of nonfatal stroke. The risk of hospitalization for heart failure (HHF) decreased in all three SGLT2i trials, and one GLP-1RA trial showed an increase in risk of HHF. The risk reduction of HHF in SGLT2i trials was greater than that in GLP-1RA trials. These findings were consistent with current systematic reviews and meta-analyses. The risk reduction of 3P-MACE was significantly and negatively correlated with changes in HbA1c (R = -0.861, P = 0.006) and body weight (R = -0.895, P = 0.003) in GLP-1RA and SGLT2i trials. The studies using SGLT2i failed to reduce carotid intima media thickness (cIMT), the surrogate marker for atherosclerosis; however, several studies using GLP-1RA successfully reduced cIMT in patients with type 2 diabetes. Compared with SGLT2i, GLP-1RA had a higher probability of decreasing serum triglyceride. GLP-1RA have multiple vascular biological anti-atherogenic properties.
Keywords: Atherosclerotic cardiovascular disease; Carotid intima media thickness; Glucagon-like peptide 1 receptor agonists; Sodium-glucose cotransporter 2 inhibitors; Triglyceride; Vascular biology
| Introduction | ▴Top |
Glucagon-like peptide 1 receptor agonists (GLP-1RA) increase pancreatic insulin secretion and decrease glucagon in glucose-dependent manner, and delay gastric emptying which suppress postprandial hyperglycemia and appetite, resulting in reduction of energy intake and body weight [1-3]. The gut-brain hormone, GLP-1 has received immense attention over the last couple of decades for its widespread metabolic effects. Intestinal GLP-1 is an endogenous satiation signal, whose eating effects are primarily mediated by vagal afferents [4]. However, the central mechanisms processing the vagal anorexigenic signals remain largely unknown. Despite the successful therapeutic use of GLP-1RA as anti-obesity drugs, the eating effects of intestinal GLP-1 still remain to be elucidated [4].
Beyond improving hemoglobin A1c (HbA1c) in adults with type 2 diabetes, GLP-1RA including dulaglutide (used in REWIND), liraglutide (used in LEADER) and subcutaneous semaglutide (used in SUSTAIN-6) have been approved for reducing risk of major adverse cardiovascular events (MACE) with established cardiovascular disease (CVD) or multiple CV risk factors [5-7]. Recently, CV outcomes of once-daily oral semaglutide was assessed (PIONEER-6) [8]. Oral semaglutide reduced MACE as compared with placebo (hazard ratio (HR): 0.79; 95% confidence interval (CI): 0.57 to 1.11; P < 0.001). However, among patients with type 2 diabetes with or without previous CVD, the incidence of MACE did not differ significantly between patients who received exenatide and those who received placebo (HR: 0.91; 95% CI: 0.83 to 1.00) in the EXSCEL study [9].
Sodium-glucose cotransporter 2 inhibitors (SGLT2i) (empagliflozin and canagliflozin) also reduced the risk for the primary composite CV outcome in patients with type 2 diabetes at high risk for CV events [10, 11]. One of SGLT2i, dapagliflozin did not result in a lower rate of MACE (HR: 0.93; 95% CI: 0.84 to 1.03; P = 0.17) but did result in a lower rate of CV death or hospitalization for heart failure (HHF) (HR: 0.83; 95% CI: 0.73 to 0.95; P = 0.005), which reflected a lower rate of HHF (HR: 0.73; 95% CI: 0.61 to 0.88); there was no between-group difference in CV death (HR: 0.98; 95% CI: 0.82 to 1.17) [12].
The American Diabetes Association (ADA) and European Association of Study in Diabetes (EASD) consensus report 2019 recommended using SGLT2i or GLP-1RA as a second-line drug after metformin or as a first-line drug in patients with diabetes with established CVD, respectively [2]. Such recommendation is based on the findings of recently concluded CV outcome trials. However, it has not yet clearly known whether GLP-1RA and SGLT2i had a similar impact on MACE. The benefit in MACE reduction with SGLT2i has been primarily derived from the reduction of CV death due to a significant decrease in HHF. In the ADA/EASD consensus report 2022 [13], there is the following description. In people with established atherosclerotic CVD (ASCVD) or with a high risk for ASCVD, GLP-1RA were prioritized over SGLT2i [13]. Given their favorable drug class effect in reducing HHF and progression of chronic kidney disease (CKD), SGLT2i were prioritized in people with HF, particularly those with a reduced ejection fraction, or CKD. We studied the superiority of GLP-1RA over SGLT2i for prevention of ASCVD which was described in the ADA/EASD consensus report 2022, from various viewpoints.
| The Association Between Risk Reduction of MACE and Changes in ASCVD Risk Factors | ▴Top |
Risk reduction of three-point MACE (3P-MACE) in GLP-1RA and SGLT2i trials
The 3P-MACE (CV death, nonfatal myocardial infarction (MI), or ischemic stroke) may reflect the development of ASCVD. The risk reduction in 3P-MACE in GLP-1RA and SGLT2i trials is shown in Figure 1. GLP-1RA, liraglutide (LAEADER), subcutaneous semaglutide (SUSTAIN-6), dulaglutide (REWIND) and oral semaglutide (PIONEER-6) reduced 3P-MACE by 13%, 26%, 12% and 21%, respectively [5-8]. Risk reduction of 3P-MACE by exenatide (EXSCEL) was 9% [9].
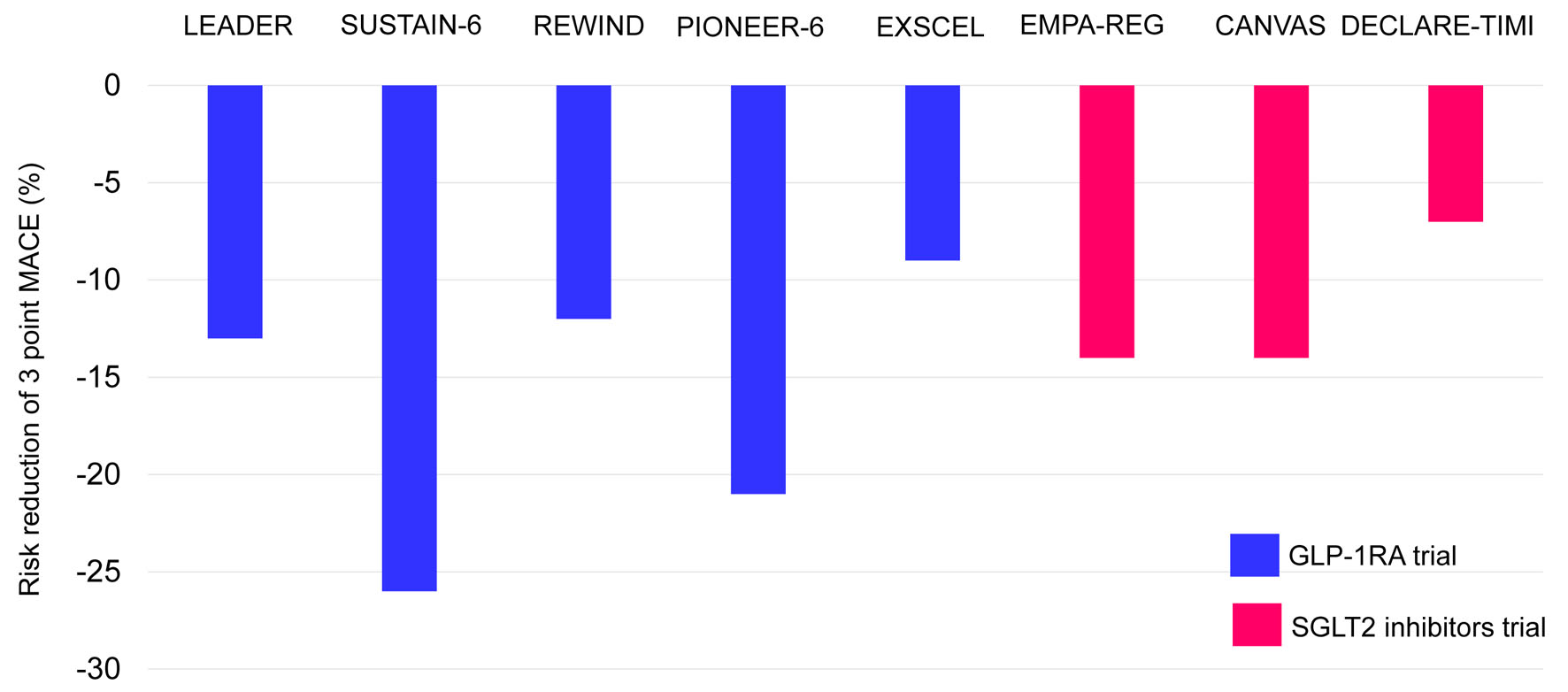 Click for large image | Figure 1. The risk reduction in three-point MACE in GLP-1RA and SGLT2i trials. MACE: major adverse cardiovascular events; GLP-1RA: glucagon-like peptide 1 receptor agonists; SGLT2i: sodium-glucose cotransporter 2 inhibitors. |
SGLT2i such as empagliflozin (EMPA-REG) and canagliflozin (CANVAS program) reduced 3P-MACE by 14% and 14%, respectively [10, 11]. Risk reduction of 3P-MACE by dapagliflozin (DECLARE-TIMI) was 7% [9].
The network meta-analysis including a total of 21 trials with 170,930 participants showed that both GLP-1RA and SGLT2i were associated with lower risks of 3P-MACE than placebo (relative risk (RR): 0.89; 95% CI: 0.84 to 0.94 and RR: 0.88; 95% CI: 0.83 to 0.94, respectively) [14]. A comparison between SGLT2i and GLP-1RA demonstrated no difference in their risks of 3P-MACE (RR: 0.99; 95% CI: 0.91 to 1.08).
The association of the risk reduction of 3P-MACE with changes in HbA1c, body weight and systolic blood pressure
The correlation between the risk reduction of 3P-MACE between changes in HbA1c is shown in Figure 2a. The risk reduction of 3P-MACE was significantly and negatively correlated with changes in HbA1c (R = -0.861, P = 0.006, by Pearson’s correlation).
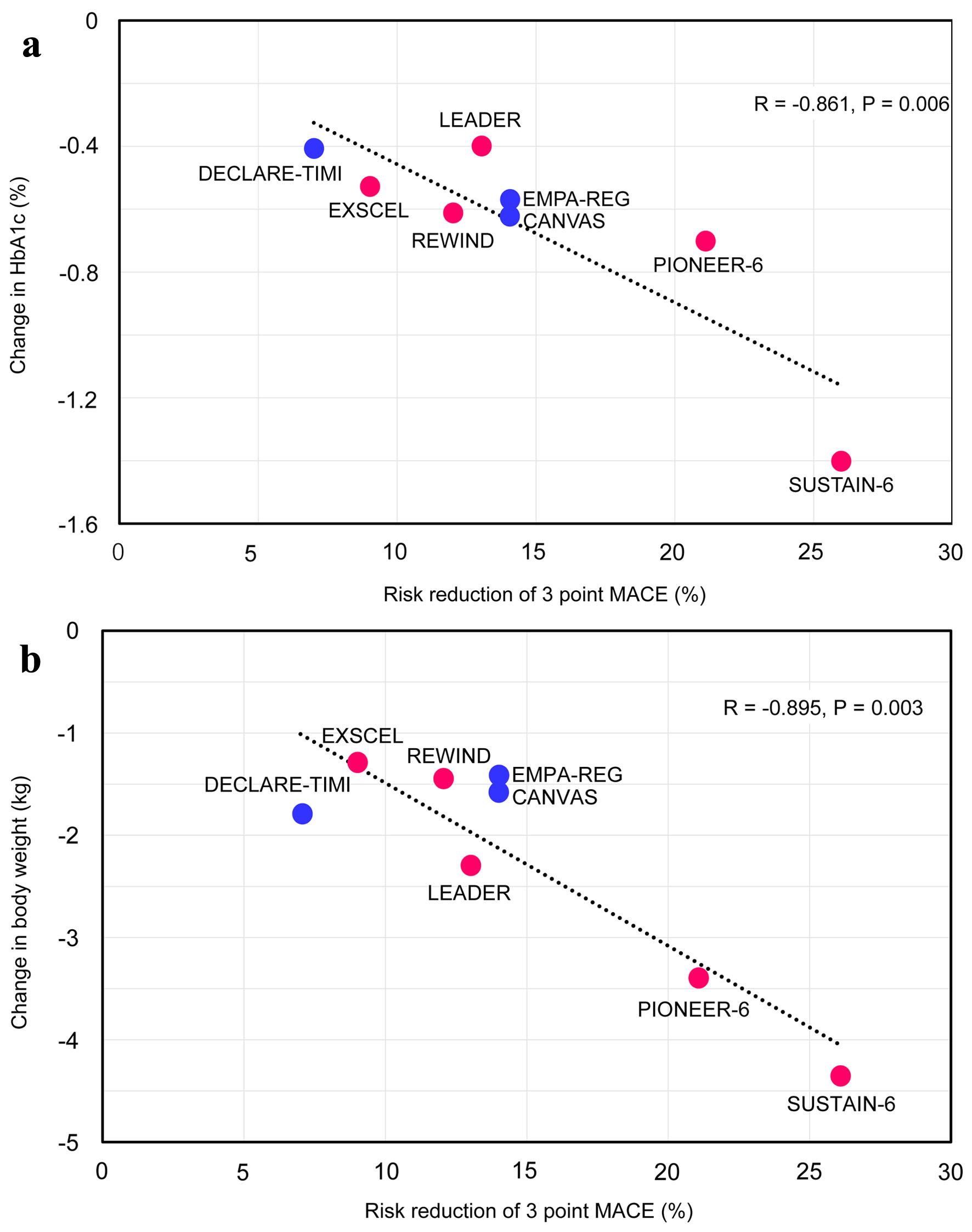 Click for large image | Figure 2. The correlation between the risk reduction of three-point MACE between changes in HbA1c (a) and body weight (b). MACE: major adverse cardiovascular events. |
The correlation between the risk reduction of 3P-MACE between changes in body weight is shown in Figure 2b. The risk reduction of 3P-MACE was significantly and negatively correlated with changes in body weight (R = -0.895, P = 0.003).
Changes in HbA1c was significantly and positively correlated with changes in body wight (R = 0.799, P = 0.017). Besides HbA1c and body weight, systolic blood pressure was the only ASCVD risk factor for which achieved value after trial was available in the eight trials. The risk reduction of 3P-MACE was not correlated with changes in systolic blood pressure (R = -0.235, P = 0.575). Changes in systolic blood pressure were correlated with changes in neither HbA1c nor body weight.
Decreases in HbA1c and body weight were significantly associated with risk reduction of 3P-MACE in GLP-1RA and SGLT2i trials.
The risk reduction of death from any cause, death from CV cause, nonfatal MI, nonfatal stroke and HHF in GLP-1RA and SGLT2i trials
The risk reduction in death from any cause, death from CV cause, nonfatal MI, nonfatal stroke and HHF in GLP-1RA and SGLT2i trials is shown in Figure 3a-e.
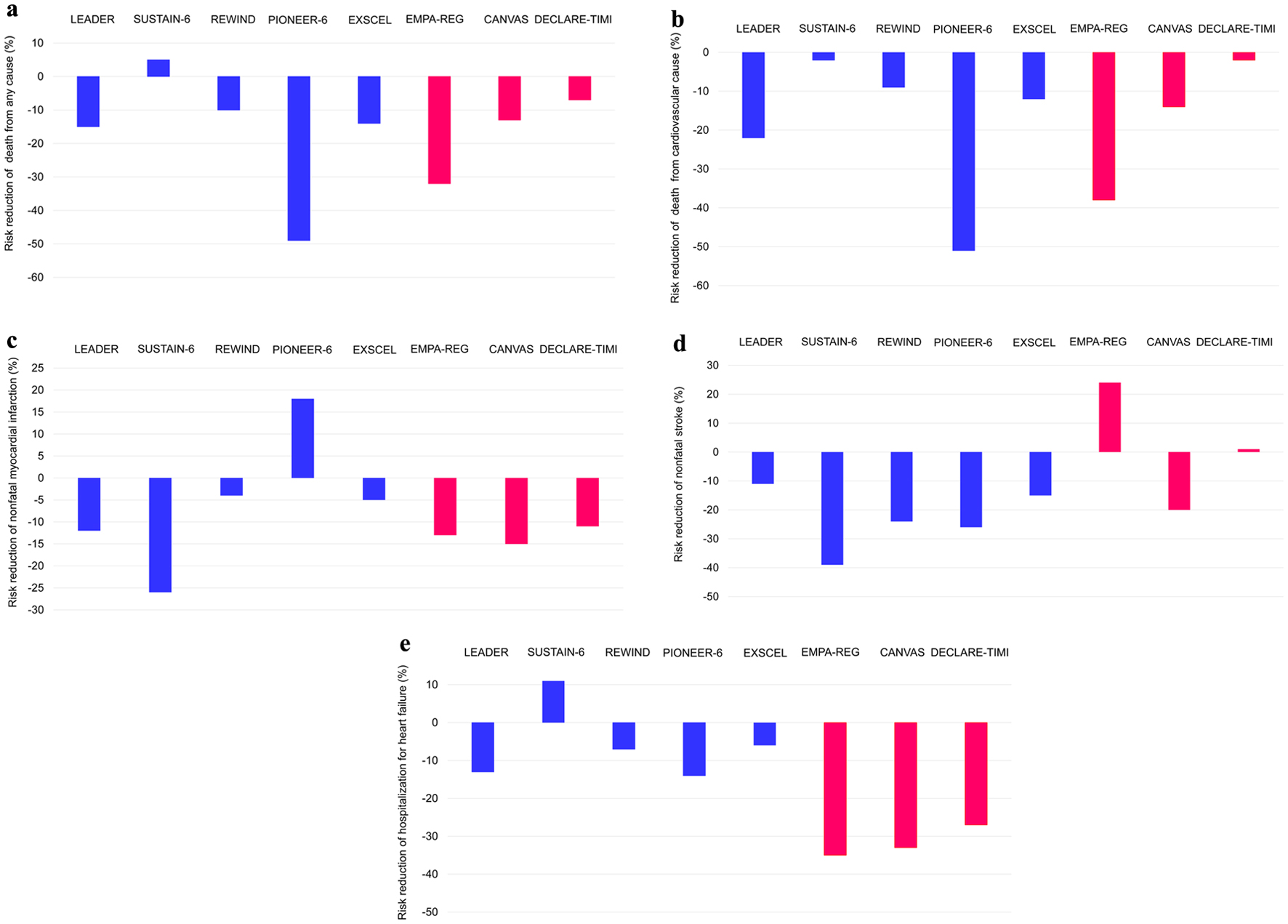 Click for large image | Figure 3. The risk reduction in death from any cause (a), death from cardiovascular cause (b), nonfatal myocardial infarction (c), nonfatal stroke (d) and hospitalization for heart failure (e) in GLP-1RA and SGLT2i trials. The data on risk reduction of nonfatal myocardial infarction and stroke in DECLARE-TIMI indicate the risk reduction in myocardial infarction including fatal myocardial infarction and stroke including fatal stroke due to the lack of data on nonfatal myocardial infarction and stroke in DECLARE-TIMI. GLP-1RA: glucagon-like peptide 1 receptor agonists; SGLT2i: sodium-glucose cotransporter 2 inhibitors. |
We could not find a meaningful difference in the risk reduction in mortality due to any cause, mortality due to CV cause and nonfatal MI between GLP-1RA and SGLT2i trials. The risk of nonfatal stroke decreased in all five GLP-1RA trials; however, two of three SGLT2i trials showed an increase in risk of nonfatal stroke. The risk of HHF decreased in all three SGLT2i trials, one GLP-1RA trial showed an increase in risk of HHF. The risk reduction of HHF in all three SGLT2i trials was greater than that in GLP-1RA trials.
The network meta-analysis showed that only GLP-1RA were associated with a lower risk of stroke compared with placebo (RR: 0.85; 95% CI: 0.76 to 0.94) [14]. SGLT2i were superior to GLP-1RA in reducing HHF (RR: 0.76; 95% CI: 0.68 to 0.84) and renal outcomes (RR: 0.78; 95% CI: 0.65 to 0.93) [14]. In a systematic review and network meta-analysis including 453 trials assessing 21 antidiabetic interventions from nine drug classes, odds of stroke were lower with subcutaneous semaglutide and dulaglutide [15]. SGLT2i reduced HHF and end-stage renal disease [15]. Another systematic review and network meta-analysis of trials showed that both classes of drugs lowered all-cause mortality, CV mortality, and nonfatal MI [16]. Notable differences were found between the two agents: SGLT-2i reduced HHF more than GLP-1RA, and GLP-1RA reduced nonfatal stroke more than SGLT-2i [16], which was consistent with our results.
Patorno et al performed a population-based study of more than 360,000 patients with diabetes, including more than 100,000 with established CVD, and found that initiating SGLT2i as compared to GLP-1RA was associated with no significant differences in the primary outcome of hospitalization for MI or stroke [17]. The rates of MI and stroke were similar in patients without history of CVD prescribed SGLT2i and GLP-1RA. The meaningful differences in the risk of all-cause mortality in those who initiated SGLT2i as compared to GLP-1RA were not observed [17].
What is urgently needed to do in the field is to conduct clinical trials to directly compare the treatment effect of the two drug classes in ASCVD in patients with type 2 diabetes.
The association of the risk reduction of death from any cause, death from CV cause, nonfatal MI, nonfatal stroke and HHF with changes in HbA1c, body weight and systolic blood pressure
The risk reduction of death from any cause, death from CV cause, nonfatal MI, nonfatal stroke and HHF was not significantly correlated with changes in HbA1c, body weight and systolic blood pressure.
| Effects of GLP-1RA and SGLT2i on the Surrogate Marker for Atherosclerosis | ▴Top |
Increased carotid intima media thickness (cIMT) is a relatively simple, inexpensive, and reproducible noninvasive marker of ASCVD. Several large prospective studies have evaluated the usefulness of ultrasonographic measurement of cIMT and have demonstrated its role in predicting future CV events [18]. Only two studies were performed to evaluate the effect of SGLT2i on cIMT. Twenty-four months of ipragliflozin treatment did not affect cIMT status in patients with type 2 diabetes, relative to the non-SGLT2i-use standard care for type 2 diabetes [19]. No cIMT changes were also observed between the tofogliflozin and the conventional treatment groups [20].
One of GLP-1RA, exenatide, more significantly reduced the cIMT from baseline compared with insulin after 52 weeks, with a mean difference of -0.14 mm (95% CI: -0.25 to -0.02; P = 0.016), in patients with type 2 diabetes [21]. There was a significant reduction in cIMT by the 18-month treatment using GLP-1RA, liraglutide, in diabetic patients with the metabolic syndrome [22]. Eight months of liraglutide use in patients with type 2 diabetes significantly reduced cIMT [23]. Liraglutide decreased cIMT after 8 months treatment independently of its effect on plasma glucose and lipids concentrations in patients with type 2 diabetes [24].
The studies using SGLT2i failed to reduce cIMT; however, several studies using GLP-1RA successfully reduced cIMT in patients with type 2 diabetes.
| Effects of GLP-1RA and SGLT2i on ASCVD Risk Factors | ▴Top |
Blood pressure
The meta-analysis which investigated effects of SGLT2i on blood pressure showed that SGLT2i reduce systolic and diastolic blood pressure by -2.46 mm Hg (95% CI: -2.28 to -2.18) and -2.23 mm Hg (95% CI: -0.78 to -0.66) [25]. The meta-analysis to synthesize current evidence for the effects of exenatide and liraglutide on blood pressure showed that GLP-1RA decreased systolic and diastolic blood pressure by -1.79 mm Hg (95% CI: -2.94 to -0.64) and -0.54 mm Hg (95% CI: -1.15 to 0.07) compared to placebo [26]. In the meta-analysis including a total of 16 randomized controlled trials (RCTs) that enrolled 3,443 patients in the GLP-1RA treatment group and 2,417 subjects in the control group [27], the GLP-1RA, exenatide, reduced systolic blood pressure when compared with placebo with mean differences of -5.24 mm Hg (95% CI: -6.88 to -3.59). In the exenatide-treated group, diastolic blood pressure was reduced by -5.91 mm Hg (95% CI: -7.53 to -4.28). Daily 1.2 mg of liraglutide treatment reduced systolic blood pressure compared with placebo with mean differences of -5.60 mm Hg (95% CI: -5.84 to -5.36). Daily 1.8 mg liraglutide also reduced systolic blood pressure compared with placebo with mean differences of -4.49 mm Hg (95% CI: -4.73 to -4.26). In the meta-analysis including 33 trials (12,469 patients), GLP-1RA treatment achieved a greater systolic blood pressure reduction than comparator therapy (weighted mean difference (WMD), -2.22 mm Hg; 95% CI: -2.97 to -1.47) [28].
The network meta-analysis evaluated comparative efficacy and safety of once-weekly GLP-1RA, semaglutide and SGLT2i in type 2 diabetes patients inadequately controlled with metformin was performed [29]. Systolic blood pressure reduction was not statistically differentiable. In another network meta-analysis including 48 publications representing 21 trials, once-weekly semaglutide was not statistically differentiable than all SGLT2i in reducing systolic blood pressure [30].
Both GLP-1RA and SGLT2i reduce blood pressure in patients with type 2 diabetes. However, regarding blood pressure-lowering, no difference was observed between GLP-1RA and SGLT2i.
Serum lipids
The information about changes in serum lipids including triglyceride (TG), total cholesterol (TC), low-density lipoprotein-cholesterol (LDL-C) and high-density lipoprotein-cholesterol (HDL-C) after the GLP-1RA and SGLT2i treatment was obtained from the meta-analyses of RCTs [25, 31-35].
The changes in serum lipids by GLP-1RA and SGLT2i are shown in Figure 4 [25, 31-35]. Reduction of TG was greater in GLP-1R treatment than in SGLT2i treatment. GLP-1RA reduced LDL-C and TC, while SGLT2i increased LDL-C and TC. Although the difference between the two drugs is small, increase of HDL-C was greater in SGLT2i treatment than in GLP-1R treatment.
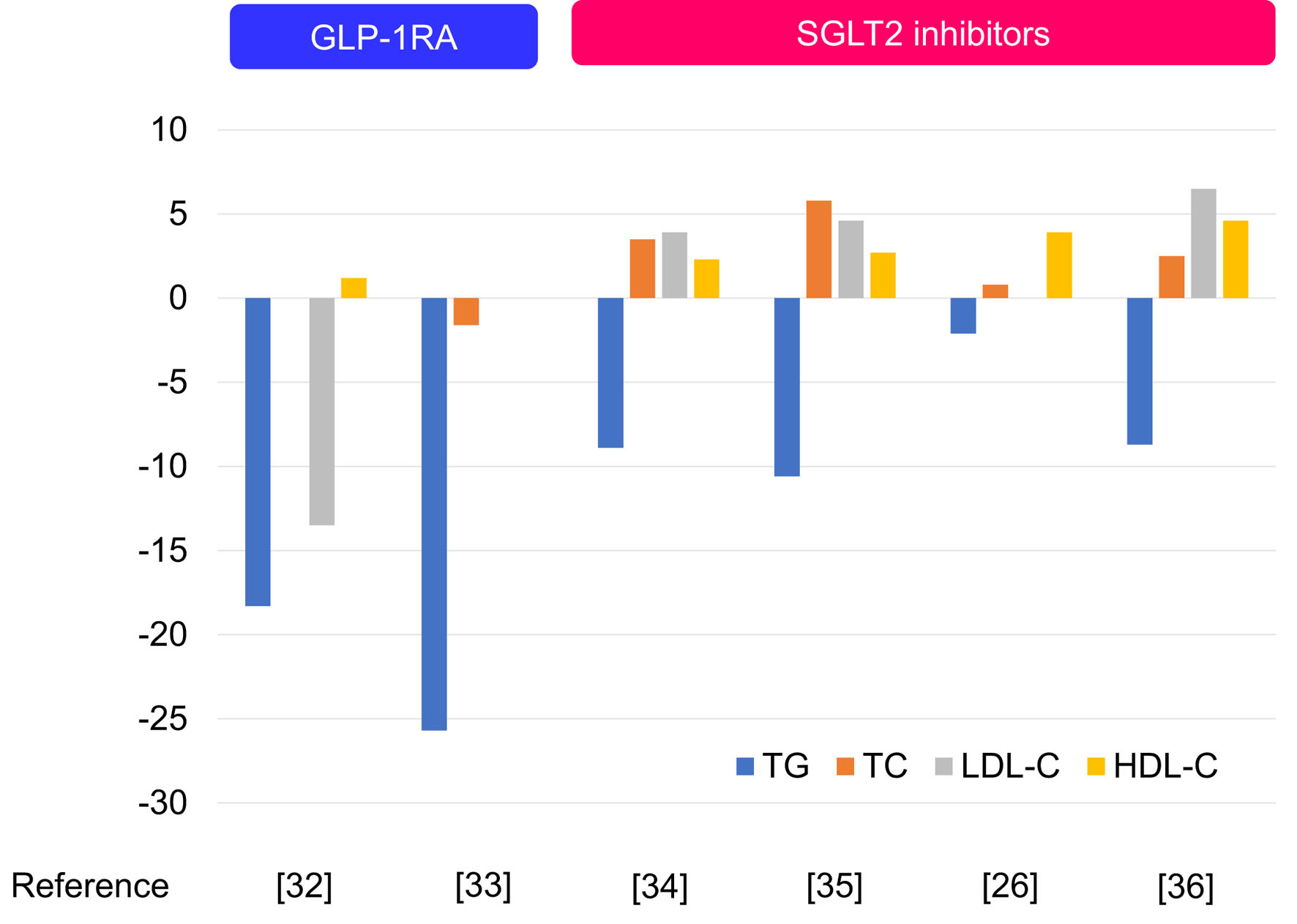 Click for large image | Figure 4. The changes in serum lipids by GLP-1RA and SGLT2i. GLP-1RA: glucagon-like peptide 1 receptor agonists; SGLT2i: sodium-glucose cotransporter 2 inhibitors. |
To evaluate and compare the ability of GLP-1RA and SGLT2i to ameliorate insulin resistance of nonalcoholic fatty liver disease (NAFLD) patients, the meta-analysis including 25 studies with 1,595 patients was performed [36]. Compared with SGLT2i, GLP-1RA had a higher probability of decreasing TG (MD: -54.0 mg/dL; 95% CI: -93.5 to -16.7). However, there was no difference between GLP-1RA and SGLT2i in effect on TC (MD: 3.5 mg/dL; 95% CI: -22.0 to 29.0). Compared with SGLT2i, GLP-1RA showed no difference in effects on HDL-C (MD: -2.8 mg/dL; 95% CI: -8.8 to 4.6) or LDL-C (MD: 2.4 mg/dL; 95% CI: -15.6 to 19.8).
| Vascular Biological Anti-Atherogenic Properties of GLP-1RA | ▴Top |
Vascular biological anti-atherogenic properties of GLP-1RA are shown in Figure 5. GLP-1RA attenuate endothelial cell dysfunction in diabetic patients and inhibit tumor necrosis factor-alpha (TNF-α)-mediated plasminogen activator inhibitor type-1 (PAI-1) induction in human vascular endothelial cells [37]. Liraglutide, a long-acting GLP-1RA, inhibited TNF-α or hyperglycemia-mediated induction of PAI-1, intercellular adhesion molecule-1 (ICAM-1) and vascular cell adhesion molecule-1 (VCAM-1) mRNA and protein expression in a human vascular endothelial cell line [38]. Endothelial nitric oxide synthase (eNOS), which synthesizes nitric oxide (NO) in endothelial cells, plays an important role in regulating various anti-atherogenesis, including vasorelaxation, the inhibition of leukocyte-endothelial adhesion, vascular smooth muscle cell migration and proliferation, and platelet aggregation [39-41]. Type 2 diabetes can lead to the reduction of NO production. GLP-1 upregulated the activity and protein expression of eNOS in human umbilical vein endothelial cells through the GLP-1R-dependent pathway [42]. Liraglutide reduced production of reactive oxygen species (ROS) and inflammation in endothelial cells with inhibition of protein kinase C alpha (PKC-α), NADPH oxidase, and nuclear factor-κB (NF-κB) signaling and upregulation of protective anti-oxidative enzymes, superoxide dismutase 2 (SOD-2) [43].
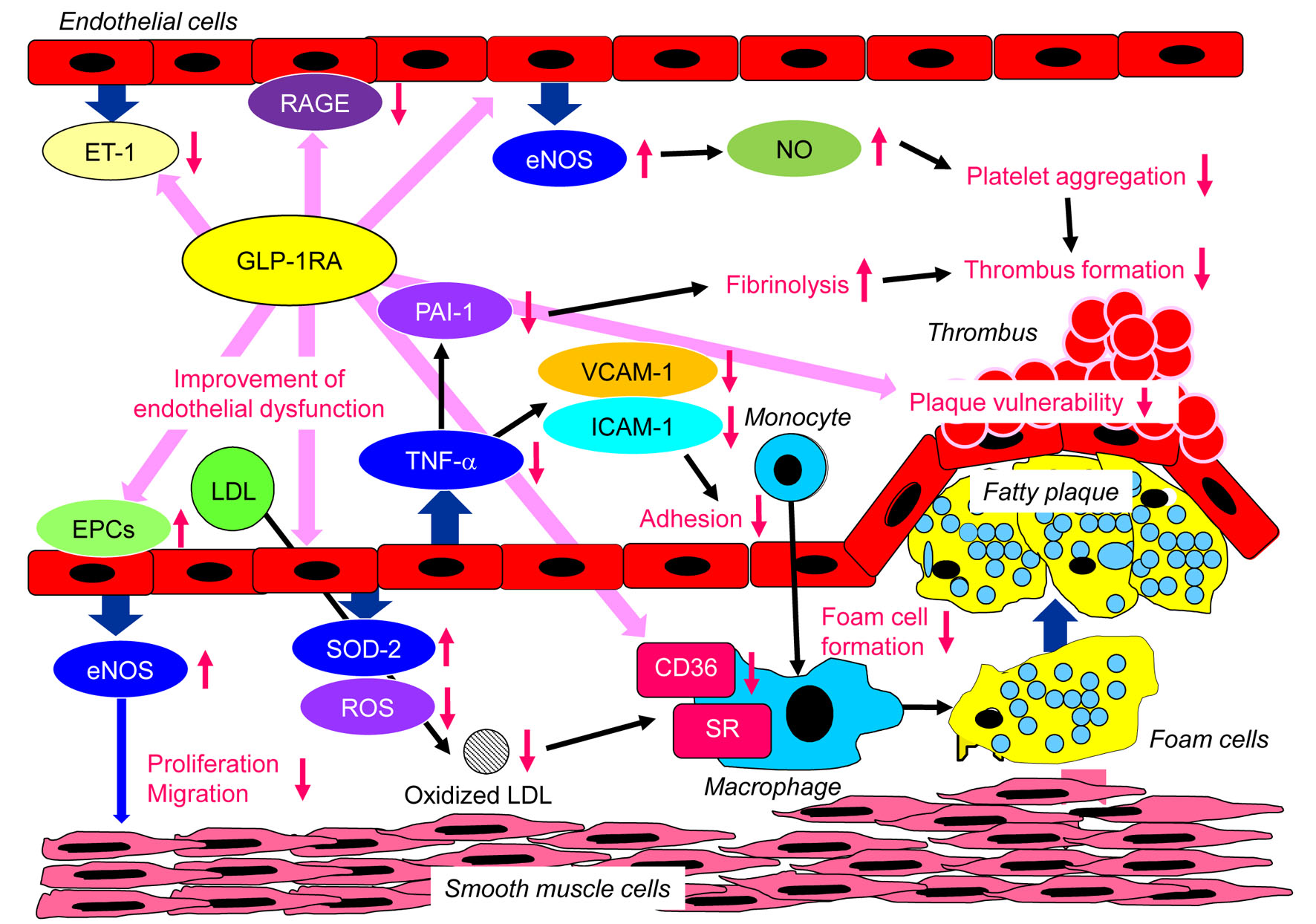 Click for large image | Figure 5. Vascular biological anti-atherogenic properties of GLP-1RA. eNOS: endothelial nitric oxide synthase; EPCs: endothelial progenitor cells; ET-1: endothelin-1; ICAM-1: intercellular adhesion molecule-1; NO: nitric oxide; PAI-1: plasminogen activator inhibitor type-1; RAGE: receptor for advanced glycation end products; ROS: reactive oxygen species; SOD-2: superoxide dismutase 2; SR: scavenger receptor; TNF-α: tumor necrosis factor-alpha; VCAM-1: vascular cell adhesion molecule-1; GLP-1RA: glucagon-like peptide 1 receptor agonists. |
Endothelial dysfunction is a very early event in diabetes and atherosclerosis, and is in part characterized by enhanced endothelin-1 (ET-1) and diminished eNOS expression, and ET-1 produced by endothelial cells is a potent vasoconstrictor whereas eNOS induces intense vasodilatation through NO synthesis [44, 45]. The balance between ET-1 and eNOS expression maintains normal function of endothelial cells. Liraglutide suppressed ET-1 expression by inhibiting the phosphorylation of NF-κB [46].
Macrophage foam cell formation, characterized by cholesterol ester accumulation catalyzed by acyl-CoA:cholesterol acyltransferase 1 (ACAT1), is the hallmark of early atherogenesis. The infusion of liraglutide into apoE(-/-) mice significantly retarded atherosclerotic lesions with monocyte/macrophage infiltration in the aortic wall and suppressed foam cell formation and ACAT1 expression in macrophages, indicating that liraglutide prevented the development of atherosclerotic lesions by suppressing macrophage foam cell formation due to ACAT1 down-regulation [47]. Liraglutide inhibited oxidized LDL uptake through protein kinase A (PKA)/CD36 pathway in macrophages [48]. Adiponectin signaling through adaptor protein PH domain and leucine zipper containing 1 (APPL1) is necessary to exert its anti-inflammatory and cytoprotective effects on endothelial cells [49, 50]. GLP-1 promotes the secretion of adiponectin which exerts anti-inflammatory effects through APPL1. GLP-1 can prevent atherosclerosis progression and plaque vulnerability in patients with type 2 diabetes, by inducing adiponectin/APPL1 signaling [51].
The formation and accumulation of advanced glycation end products (AGEs) progress under diabetic conditions. Accumulating evidence has suggested that receptor for AGEs (RAGE) serves a pivotal role in promoting inflammatory processes and endothelial activation, which accelerates atherosclerosis in patients with diabetes [52, 53]. Liraglutide treatment reduced serum AGEs levels, and reduced the expression of RAGE in aorta, and relieved atherosclerotic lesions compared with the control in ApoE(-/-) mice, suggesting that liraglutide serves an anti-atherosclerotic effect via inhibiting AGEs-induced RAGE expression [54].
Endothelial progenitor cells (EPCs) are derived from bone marrow that can enter peripheral blood and differentiate into mature endothelial cells [55]. EPCs participate in angiogenesis in ischemic tissue and repair vascular endothelial injury [56], and EPCs are highly related to atherosclerosis [57]. A meta-analysis showed that lower EPC levels predicted a higher incidence of CV events and CV mortality in patients with diabetes [58]. Dulaglutide increased the number and function of EPCs in peripheral blood and improved arterial elasticity in patients with type 2 diabetes [59].
| Conclusion | ▴Top |
The meaningful differences in the risk reduction in 3P-MACE, mortality due to any cause, mortality due to CV cause and nonfatal MI between GLP-1RA and SGLT2i trials were not observed. Notable differences were found between the two agents: SGLT2i reduced HHF more than GLP-1RA, and GLP-1RA reduced nonfatal stroke more than SGLT-2i. The SGLT2i trials failed to reduce IMT; however, several GLP-1RA trials successfully reduced IMT in patients with type 2 diabetes. GLP-1RA have multiple vascular biological anti-atherogenic properties.
Acknowledgments
We thank the staffs of the Division of Research Support, National Center for Global Health and Medicine Kohnodai Hospital.
Financial Disclosure
Authors have no financial disclosure to report.
Conflict of Interest
The authors declare that they have no conflict of interest concerning this article.
Author Contributions
HY designed the research, and MH, HA and HK collected and analyzed data. HY wrote and approved the final paper.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
| References | ▴Top |
- Davies MJ, D'Alessio DA, Fradkin J, Kernan WN, Mathieu C, Mingrone G, Rossing P, et al. Management of hyperglycaemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia. 2018;61(12):2461-2498.
doi pubmed - Buse JB, Wexler DJ, Tsapas A, Rossing P, Mingrone G, Mathieu C, D'Alessio DA, et al. 2019 update to: Management of hyperglycaemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia. 2020;63(2):221-228.
doi pubmed - Nauck MA, Quast DR, Wefers J, Meier JJ. GLP-1 receptor agonists in the treatment of type 2 diabetes - state-of-the-art. Mol Metab. 2021;46:101102.
doi pubmed - Krieger JP. Intestinal glucagon-like peptide-1 effects on food intake: Physiological relevance and emerging mechanisms. Peptides. 2020;131:170342.
doi pubmed - Gerstein HC, Colhoun HM, Dagenais GR, Diaz R, Lakshmanan M, Pais P, Probstfield J, et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): a double-blind, randomised placebo-controlled trial. Lancet. 2019;394(10193):121-130.
doi pubmed - Marso SP, Daniels GH, Brown-Frandsen K, Kristensen P, Mann JF, Nauck MA, Nissen SE, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2016;375(4):311-322.
doi pubmed - Marso SP, Bain SC, Consoli A, Eliaschewitz FG, Jodar E, Leiter LA, Lingvay I, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375(19):1834-1844.
doi pubmed - Husain M, Birkenfeld AL, Donsmark M, Dungan K, Eliaschewitz FG, Franco DR, Jeppesen OK, et al. Oral semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2019;381(9):841-851.
doi pubmed - Holman RR, Bethel MA, Mentz RJ, Thompson VP, Lokhnygina Y, Buse JB, Chan JC, et al. Effects of once-weekly exenatide on cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2017;377(13):1228-1239.
doi pubmed - Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, Mattheus M, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373(22):2117-2128.
doi pubmed - Neal B, Perkovic V, Mahaffey KW, de Zeeuw D, Fulcher G, Erondu N, Shaw W, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377(7):644-657.
doi pubmed - Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, Silverman MG, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380(4):347-357.
doi pubmed - Davies MJ, Aroda VR, Collins BS, Gabbay RA, Green J, Maruthur NM, Rosas SE, et al. Management of hyperglycemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2022;45(11):2753-2786.
doi pubmed - Lin DS, Lee JK, Hung CS, Chen WJ. The efficacy and safety of novel classes of glucose-lowering drugs for cardiovascular outcomes: a network meta-analysis of randomised clinical trials. Diabetologia. 2021;64(12):2676-2686.
doi pubmed - Tsapas A, Avgerinos I, Karagiannis T, Malandris K, Manolopoulos A, Andreadis P, Liakos A, et al. Comparative effectiveness of glucose-lowering drugs for type 2 diabetes: a systematic review and network meta-analysis. Ann Intern Med. 2020;173(4):278-286.
doi pubmed - Palmer SC, Tendal B, Mustafa RA, Vandvik PO, Li S, Hao Q, Tunnicliffe D, et al. Sodium-glucose cotransporter protein-2 (SGLT-2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists for type 2 diabetes: systematic review and network meta-analysis of randomised controlled trials. BMJ. 2021;372:m4573.
- Patorno E, Htoo PT, Glynn RJ, Schneeweiss S, Wexler DJ, Pawar A, Bessette LG, et al. Sodium-glucose cotransporter-2 inhibitors versus glucagon-like peptide-1 receptor agonists and the risk for cardiovascular outcomes in routine care patients with diabetes across categories of cardiovascular disease. Ann Intern Med. 2021;174(11):1528-1541.
doi pubmed - Sinha AK, Eigenbrodt M, Mehta JL. Does carotid intima media thickness indicate coronary atherosclerosis? Curr Opin Cardiol. 2002;17(5):526-530.
doi pubmed - Tanaka A, Sata M, Okada Y, Teragawa H, Eguchi K, Shimabukuro M, Taguchi I, et al. Effect of ipragliflozin on carotid intima-media thickness in patients with type 2 diabetes: a multicenter, randomized, controlled trial. Eur Heart J Cardiovasc Pharmacother. 2023;9(2):165-172.
doi pubmed - Katakami N, Mita T, Yoshii H, Shiraiwa T, Yasuda T, Okada Y, Torimoto K, et al. Tofogliflozin does not delay progression of carotid atherosclerosis in patients with type 2 diabetes: a prospective, randomized, open-label, parallel-group comparative study. Cardiovasc Diabetol. 2020;19(1):110.
doi pubmed - Zhang J, Xian TZ, Wu MX, Li C, Pan Q, Guo LX. Comparison of the effects of twice-daily exenatide and insulin on carotid intima-media thickness in type 2 diabetes mellitus patients: a 52-week randomized, open-label, controlled trial. Cardiovasc Diabetol. 2020;19(1):48.
doi pubmed - Rizzo M, Rizvi AA, Patti AM, Nikolic D, Giglio RV, Castellino G, Li Volti G, et al. Liraglutide improves metabolic parameters and carotid intima-media thickness in diabetic patients with the metabolic syndrome: an 18-month prospective study. Cardiovasc Diabetol. 2016;15(1):162.
doi pubmed - Rizvi AA, Patti AM, Giglio RV, Nikolic D, Amato A, Al-Busaidi N, Al-Rasadi K, et al. Liraglutide improves carotid intima-media thickness in patients with type 2 diabetes and non-alcoholic fatty liver disease: an 8-month prospective pilot study. Expert Opin Biol Ther. 2015;15(10):1391-1397.
doi pubmed - Rizzo M, Chandalia M, Patti AM, Di Bartolo V, Rizvi AA, Montalto G, Abate N. Liraglutide decreases carotid intima-media thickness in patients with type 2 diabetes: 8-month prospective pilot study. Cardiovasc Diabetol. 2014;13:49.
doi pubmed - Mazidi M, Rezaie P, Gao HK, Kengne AP. Effect of sodium-glucose cotransport-2 inhibitors on blood pressure in people with type 2 diabetes mellitus: a systematic review and meta-analysis of 43 randomized control trials with 22 528 patients. J Am Heart Assoc. 2017;6(6):e004007.
doi pubmed - Robinson LE, Holt TA, Rees K, Randeva HS, O'Hare JP. Effects of exenatide and liraglutide on heart rate, blood pressure and body weight: systematic review and meta-analysis. BMJ Open. 2013;3(1):e001986.
doi pubmed - Wang B, Zhong J, Lin H, Zhao Z, Yan Z, He H, Ni Y, et al. Blood pressure-lowering effects of GLP-1 receptor agonists exenatide and liraglutide: a meta-analysis of clinical trials. Diabetes Obes Metab. 2013;15(8):737-749.
doi pubmed - Katout M, Zhu H, Rutsky J, Shah P, Brook RD, Zhong J, Rajagopalan S. Effect of GLP-1 mimetics on blood pressure and relationship to weight loss and glycemia lowering: results of a systematic meta-analysis and meta-regression. Am J Hypertens. 2014;27(1):130-139.
doi pubmed - Sharma R, Wilkinson L, Vrazic H, Popoff E, Lopes S, Kanters S, Druyts E. Comparative efficacy of once-weekly semaglutide and SGLT-2 inhibitors in type 2 diabetic patients inadequately controlled with metformin monotherapy: a systematic literature review and network meta-analysis. Curr Med Res Opin. 2018;34(9):1595-1603.
doi pubmed - Kanters S, Wilkinson L, Vrazic H, Sharma R, Lopes S, Popoff E, Druyts E. Comparative efficacy of once-weekly semaglutide versus SGLT-2 inhibitors in patients inadequately controlled with one to two oral antidiabetic drugs: a systematic literature review and network meta-analysis. BMJ Open. 2019;9(7):e023458.
doi pubmed - Berg G, Barchuk M, Lobo M, Nogueira JP. Effect of glucagon-like peptide-1 (GLP-1) analogues on epicardial adipose tissue: A meta-analysis. Diabetes Metab Syndr. 2022;16(7):102562.
doi pubmed - Monami M, Dicembrini I, Nardini C, Fiordelli I, Mannucci E. Effects of glucagon-like peptide-1 receptor agonists on cardiovascular risk: a meta-analysis of randomized clinical trials. Diabetes Obes Metab. 2014;16(1):38-47.
doi pubmed - Sanchez-Garcia A, Simental-Mendia M, Millan-Alanis JM, Simental-Mendia LE. Effect of sodium-glucose co-transporter 2 inhibitors on lipid profile: A systematic review and meta-analysis of 48 randomized controlled trials. Pharmacol Res. 2020;160:105068.
doi pubmed - Li D, Wu T, Wang T, Wei H, Wang A, Tang H, Song Y. Effects of sodium glucose cotransporter 2 inhibitors on risk of dyslipidemia among patients with type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. Pharmacoepidemiol Drug Saf. 2020;29(5):582-590.
doi pubmed - Chen MB, Wang H, Cui WY, Xu HL, Zheng QH. Effect of SGLT inhibitors on weight and lipid metabolism at 24 weeks of treatment in patients with diabetes mellitus: A systematic review and network meta-analysis. Medicine (Baltimore). 2021;100(6):e24593.
doi pubmed - Yan H, Huang C, Shen X, Li J, Zhou S, Li W. GLP-1 RAs and SGLT-2 inhibitors for insulin resistance in nonalcoholic fatty liver disease: systematic review and network meta-analysis. Front Endocrinol (Lausanne). 2022;13:923606.
doi pubmed - Liu H, Hu Y, Simpson RW, Dear AE. Glucagon-like peptide-1 attenuates tumour necrosis factor-alpha-mediated induction of plasminogen [corrected] activator inhibitor-1 expression. J Endocrinol. 2008;196(1):57-65.
doi pubmed - Liu H, Dear AE, Knudsen LB, Simpson RW. A long-acting glucagon-like peptide-1 analogue attenuates induction of plasminogen activator inhibitor type-1 and vascular adhesion molecules. J Endocrinol. 2009;201(1):59-66.
doi pubmed - Yang Z, Ming XF. Recent advances in understanding endothelial dysfunction in atherosclerosis. Clin Med Res. 2006;4(1):53-65.
doi pubmed - Bauer V, Sotnikova R. Nitric oxide—the endothelium-derived relaxing factor and its role in endothelial functions. Gen Physiol Biophys. 2010;29(4):319-340.
doi pubmed - Stankevicius E, Kevelaitis E, Vainorius E, Simonsen U. [Role of nitric oxide and other endothelium-derived factors]. Medicina (Kaunas). 2003;39(4):333-341.
- Ding L, Zhang J. Glucagon-like peptide-1 activates endothelial nitric oxide synthase in human umbilical vein endothelial cells. Acta Pharmacol Sin. 2012;33(1):75-81.
doi pubmed - Shiraki A, Oyama J, Komoda H, Asaka M, Komatsu A, Sakuma M, Kodama K, et al. The glucagon-like peptide 1 analog liraglutide reduces TNF-alpha-induced oxidative stress and inflammation in endothelial cells. Atherosclerosis. 2012;221(2):375-382.
doi pubmed - Madden JA. Role of the vascular endothelium and plaque in acute ischemic stroke. Neurology. 2012;79(13 Suppl 1):S58-S62.
doi pubmed - Toda N, Nakanishi-Toda M. How mental stress affects endothelial function. Pflugers Arch. 2011;462(6):779-794.
doi pubmed - Dai Y, Mehta JL, Chen M. Glucagon-like peptide-1 receptor agonist liraglutide inhibits endothelin-1 in endothelial cell by repressing nuclear factor-kappa B activation. Cardiovasc Drugs Ther. 2013;27(5):371-380.
doi pubmed - Tashiro Y, Sato K, Watanabe T, Nohtomi K, Terasaki M, Nagashima M, Hirano T. A glucagon-like peptide-1 analog liraglutide suppresses macrophage foam cell formation and atherosclerosis. Peptides. 2014;54:19-26.
doi pubmed - Dai Y, Dai D, Wang X, Ding Z, Li C, Mehta JL. GLP-1 agonists inhibit ox-LDL uptake in macrophages by activating protein kinase A. J Cardiovasc Pharmacol. 2014;64(1):47-52.
doi pubmed - Mao X, Kikani CK, Riojas RA, Langlais P, Wang L, Ramos FJ, Fang Q, et al. APPL1 binds to adiponectin receptors and mediates adiponectin signalling and function. Nat Cell Biol. 2006;8(5):516-523.
doi pubmed - Wang Y, Cheng KK, Lam KS, Wu D, Wang Y, Huang Y, Vanhoutte PM, et al. APPL1 counteracts obesity-induced vascular insulin resistance and endothelial dysfunction by modulating the endothelial production of nitric oxide and endothelin-1 in mice. Diabetes. 2011;60(11):3044-3054.
doi pubmed - Barbieri M, Marfella R, Esposito A, Rizzo MR, Angellotti E, Mauro C, Siniscalchi M, et al. Incretin treatment and atherosclerotic plaque stability: Role of adiponectin/APPL1 signaling pathway. J Diabetes Complications. 2017;31(2):295-303.
doi pubmed - Huttunen HJ, Fages C, Rauvala H. Receptor for advanced glycation end products (RAGE)-mediated neurite outgrowth and activation of NF-kappaB require the cytoplasmic domain of the receptor but different downstream signaling pathways. J Biol Chem. 1999;274(28):19919-19924.
doi pubmed - Bierhaus A, Schiekofer S, Schwaninger M, Andrassy M, Humpert PM, Chen J, Hong M, et al. Diabetes-associated sustained activation of the transcription factor nuclear factor-kappaB. Diabetes. 2001;50(12):2792-2808.
doi pubmed - Li P, Tang Z, Wang L, Feng B. Glucagon-like peptide-1 analogue liraglutide ameliorates atherogenesis via inhibiting advanced glycation end product-induced receptor for advanced glycosylation end product expression in apolipoprotein-E deficient mice. Mol Med Rep. 2017;16(3):3421-3426.
doi pubmed - Qiu Y, Zhang C, Zhang G, Tao J. Endothelial progenitor cells in cardiovascular diseases. Aging Med (Milton). 2018;1(2):204-208.
doi pubmed - Chopra H, Hung MK, Kwong DL, Zhang CF, Pow EHN. Insights into endothelial progenitor cells: origin, classification, potentials, and prospects. Stem Cells Int. 2018;2018:9847015.
doi pubmed - Mudyanadzo TA. Endothelial progenitor cells and cardiovascular correlates. Cureus. 2018;10(9):e3342.
doi - Rigato M, Avogaro A, Fadini GP. Levels of circulating progenitor cells, cardiovascular outcomes and death: a meta-analysis of prospective observational studies. Circ Res. 2016;118(12):1930-1939.
doi pubmed - Xie D, Li Y, Xu M, Zhao X, Chen M. Effects of dulaglutide on endothelial progenitor cells and arterial elasticity in patients with type 2 diabetes mellitus. Cardiovasc Diabetol. 2022;21(1):200.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.