

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 14, Number 1, February 2023, pages 38-44

Potential Association of Holidays on Internationalized Normalized Ratio in Warfarin-Users at a Multidisciplinary Clinic
Rachel Ryua, c ![]() , Khaled Bahjrib, Huyentran Tranb
, Khaled Bahjrib, Huyentran Tranb
aWestern University of Health Sciences College of Pharmacy, Pomona, CA 91766, USA
bLoma Linda University School of Pharmacy, Loma Linda, CA 92350, USA
cCorresponding Author: Rachel Ryu, Western University of Health Sciences College of Pharmacy, Pomona, CA 91766, USA
Manuscript submitted November 8, 2022, accepted January 6, 2023, published online February 25, 2023
Short title: Association of Holidays and INR
doi: https://doi.org/10.14740/cr1448
| Abstract | ▴Top |
Background: Warfarin is approved by the United States Food and Drug Administration for numerous clinical indications. The effectiveness of warfarin is highly dependent on the time-in-therapeutic range based on the international normalized ratio (INR) goal, which may be altered by changes in diet, alcohol intake, concomitant drugs, and travel, all of which are prevalent during the holidays. At this time, there are no published studies assessing the impact of holidays on INR in warfarin-users.
Methods: A retrospective chart review was conducted on all adult patients taking warfarin and managed at a multidisciplinary clinic. Patients were included if they were taking warfarin at home regardless of indication for anticoagulation. The INR pre- and post-holiday was assessed.
Results: Of a total of 92 patients, the mean age was 71.5 ± 14.3 years, and most patients were on warfarin with an INR goal of 2 - 3 (89%). There were significant differences in INR before and after Independence Day (2.55 vs. 2.81, P = 0.043) and Columbus Day (2.39 vs. 2.82, P < 0.001). The remaining holidays showed no significant differences in INR before and after each respective holiday.
Conclusions: There may be factors related to Independence and Columbus Day that are increasing the level of anticoagulation in warfarin-users. Although the mean post-holiday INR values, in essence, maintained within the typical target of 2 - 3, our study underscores the specialized care that is warranted in higher risk patients to prevent a continued increase in INR and subsequent toxicities. We hope our results would be hypothesis-generating and aid in the development of larger, prospective evaluations to validate the findings of our present study.
Keywords: Cardiology; Anticoagulation; International normalized ratio; Warfarin
| Introduction | ▴Top |
Warfarin is approved by the United States (US) Food and Drug Administration for numerous clinical indications, including prophylaxis and treatment of venous thromboembolism (e.g., pulmonary embolism and deep venous thrombosis), stroke prophylaxis in atrial fibrillation, and thromboembolism prophylaxis in prosthetic cardiac valves [1]. The effectiveness of warfarin is contingent on the time-in-therapeutic range (TTR) based on the international normalized ratio (INR) goal. The desired INR range is customarily 2 - 3 but varies by indication and patient characteristics [2]. Warfarin is presumed to have reduced efficacy if the TTR is < 60-65%, and depending on the study design, patient population, and clinical use, the average TTR reported is 30-40% [2-4]. Despite the approval of several direct-acting oral anticoagulants that do not require routine INR monitoring, warfarin is still the drug of choice for various clinical settings, such as the presence of a mechanical heart valve [5].
INR is highly sensitive and affected by a multitude of factors, such as medication adherence, interacting medications or herbs, inconsistent diet of vitamin K-containing foods, alcohol intake, acute illness, liver disease, amongst a myriad of others [1, 6]. Due to warfarin’s narrow therapeutic range and copious opportunities for interactions, there is large variability in INR and therapeutic outcomes. At this time, there are no published studies assessing the impact of holidays on INR, and we believe several factors surrounding holidays may be clinically significant.
While traveling, patients may be on pharmacotherapy for malaria prophylaxis, which may lead to a supratherapeutic INR in warfarin-users; drug options for this indication include doxycycline, tetracycline, azithromycin, amoxicillin, and amoxicillin/clavulanate [1, 7]. Further, acute infections and vomiting can decrease the uptake of vitamin K and disturb the production of clotting factors, thereby affecting INR. Moreover, temperature and altitude variations encountered during travel may affect bleeding tendencies and INR [8-10]. We hypothesized that holidays may affect patients’ INR, based on possible lifestyle alterations surrounding the holiday seasons. Our primary objective was to assess the change in INR pre- and post-holidays.
| Materials and Methods | ▴Top |
A retrospective chart review was conducted on all adult patients aged 18 years and older and followed up at Loma Linda University International Heart Institute Faculty Medical Offices - Anticoagulation Clinic between January 1, 2018 through December 31, 2018. Patients were included if they were taking warfarin at home regardless of the indication for anticoagulation. The INR pre- and post-holiday was assessed, with an INR value included if there was one available within 2 weeks before and after each holiday. If there were multiple labs meeting these criteria, the INR value closest in proximity to the holiday was used. The precise timeframe of the INR collection in reference to each holiday was noted and reported. Holiday was defined as the 10 annual federal holidays recognized by the USA [11]. Patients were excluded if they were pediatric, were on other anticoagulants, or managed by an outside provider.
Information on race was collected as per the demographic information listed in the electronic medical chart. Data on the past medical history, substance use, and INR goal were gathered based on chart review. Descriptive statistics were presented for categorical variables in the form of numbers and percentages. Mean and standard deviation were used to represent the continuous variables. Paired t-tests were used to compare continuous data for pre- and post-INR. SPSS version 26 (IBM SPSS, Inc., Armonk, NY) was utilized to analyze the data with the level of significance set at α = 0.05. Missing data were handled with the deletion approach. The study was approved by the Institutional Review Board at Loma Linda University Heath. This study was conducted in compliance with the ethical standards of the responsible institution on human subjects, as well as with the Helsinki Declaration.
| Results | ▴Top |
Of a total of 92 patients, the mean age was 71.5 ± 14.3 years; patients were predominately male (55.4%) and Caucasian (62%) (Table 1 [12]). Hypertension and hyperlipidemia were the most common comorbidities (70.3% and 55.4%, respectively). Liver disease was infrequent (4.3%), and there was minimal substance use reported. Most patients were on warfarin with an INR goal of 2 - 3 (89%).
 Click to view | Table 1. Baseline Characteristics of Total Sample (n = 92) |
The mean number of days for each INR collection in relation to the holidays, as well as the calendar dates corresponding to each holiday, is presented in Table 2. There were no statistically significant differences between the mean days for the INR values with respect to the holidays. Compared to other holidays, the holiday with the longest duration for the pre- and post-holiday INR was Christmas (9.59 ± 8.83 vs. 8.53 ± 7.31, P = 0.472), and the holiday with the shortest duration for the pre- and post-holiday INR was Columbus Day (2.89 ± 5.14 vs. 3.12 ± 5.76, P = 0.802). Overall, there was great variability in the time of INR collection in reference to the holidays, as indicated by the large standard deviations.
Click to view | Table 2. Pre- and Post-Holiday INR Timeframe in Reference to Each Holiday |
Based on the results of our study, there were significant differences in INR values before and after Independence Day and Columbus Day (Table 3). The mean INR pre-Independence Day was 2.55 ± 0.71, while the mean post-INR was 2.81 ± 1.19 (P = 0.043). Most patients had an INR goal of 2 - 3 (61/65, 93.8%). With respect to Columbus Day, the mean INR pre-holiday increased from 2.39 ± 0.7 to 2.82 ± 0.89 post-holiday (P < 0.001). Again, the majority of patients’ goal INR was 2 - 3 (67/71, 94.4%). The remaining holidays showed no significant differences in INR pre- and post-holiday.
Click to view | Table 3. Pre- and Post-Holiday INR |
Regarding drug interactions with warfarin, we found 12 distinct medications with a total of 119 possible interactions (Fig. 1). The most common interacting medications were aspirin (20%) and amiodarone (18%). Concomitant interacting anti-infectives included azithromycin (n = 2), amoxicillin (n = 2), and ketoconazole (n = 1). With regard to dietary habits, there were inconsistencies in the way the data were reported in the electronic medical chart, and there was significant interpatient variability. Some patient charts stated changes in the intake of vitamin K-containing foods (36%), while others indicated no change (24%) or omitted such information (40%).
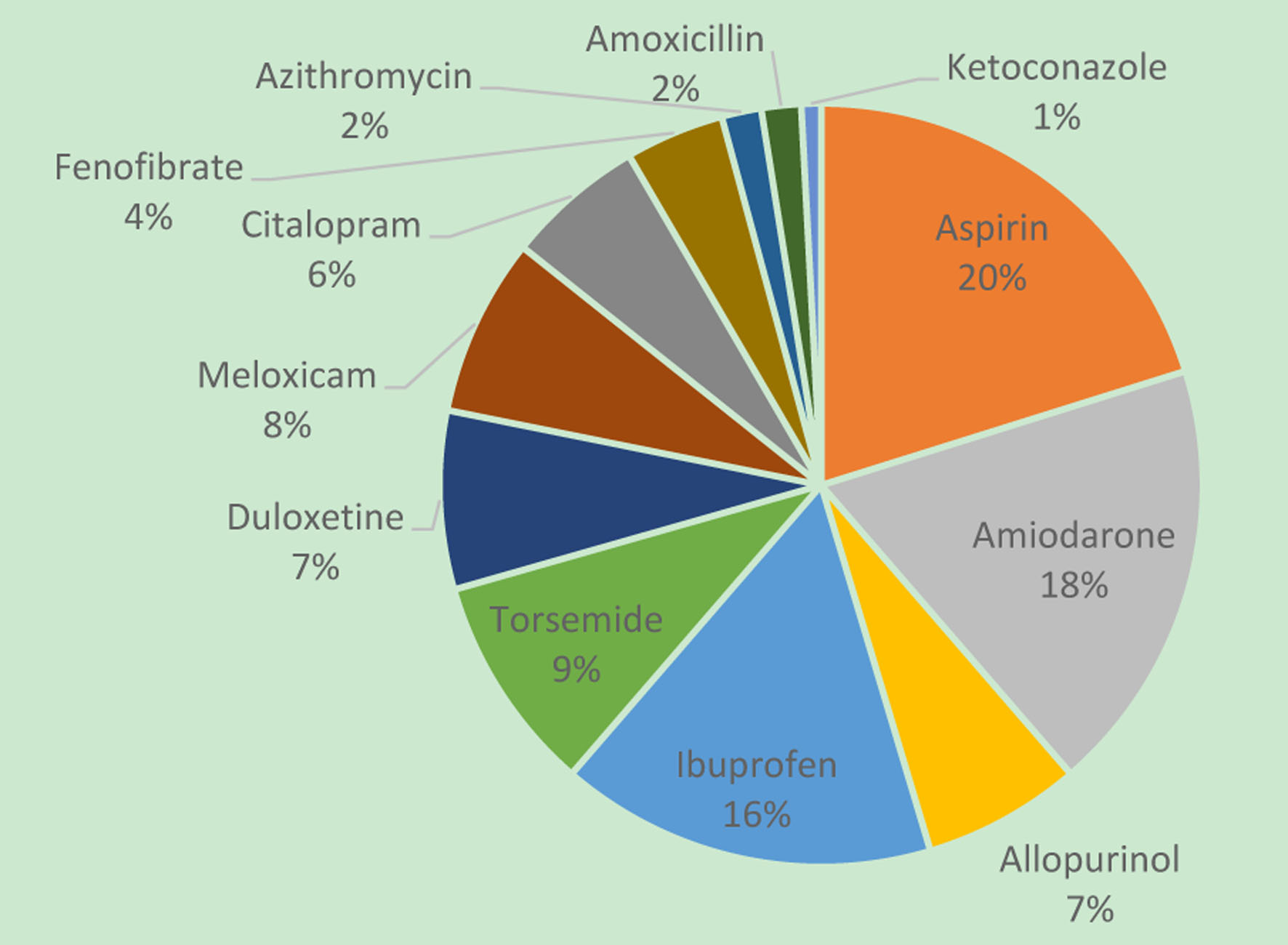 Click for large image | Figure 1. Drug interactions with warfarin. |
| Discussion | ▴Top |
Based on the results of our study, we found that Independence Day and Columbus Day had significant differences pre- and post- each respective holiday, albeit the increased INR was still deemed to be at goal per the most desired INR range of 2 - 3. According to the US Bureau of Transportation Statistics, the busiest times of long-distance travel (defined as a destination ≥ 50 miles away) are Thanksgiving, Christmas, and New Year’s [13]. As such, travel may not be a major explanation for the differences in INR observed for Independence and Columbus Day.
Independence Day is a major holiday that commemorates the independence of the USA from Great Britain [14]. It is typically celebrated with barbeques, picnics, firework displays, and festivals. Commonly consumed foods include hamburgers, hot dogs, fries, and potatoes; green vegetables are less commonly consumed, which contain vitamin K [15]. The inconsistent intake of vitamin K-containing foods is considered an interaction with warfarin, and a sudden reduction in these foods may increase the INR [1]. An increase in INR may also occur due to alcohol consumption, which is a well-known interaction [1].
There was also a significant difference in INR before and after Columbus Day, from 2.39 to 2.82. Columbus Day celebrates Christopher Columbus’s historic voyage to the Americas in 1492 [16]. Foods typically eaten include beef, pork, salted fish, rice, legumes, and desserts [17]. Similar to the traditions of Independence Day, there may be scarce opportunities to continue a consistent intake of vitamin K-containing foods for warfarin-users, potentially increasing the INR. Alcohol consumption may also play a pivotal role in affecting the INR as well.
Moreover, patients were able to obtain their INRs closest to Columbus Day, as denoted by the lowest number of mean days for the pre- and post-holiday INR in reference to the actual holiday (2.89 ± 5.14 vs. 3.12 ± 5.76 respectively, P = 0.802). It may be that more patients were available and able to complete their lab work, potentially due to lack of significant travel. The significant change in INR that was observed after Columbus Day may reveal the possibly more frequent changes in INR that could be inconspicuously occurring surrounding a holiday, which may not be as prominent if INRs were obtained more remotely from the actual holiday; longer gaps in attaining post-holiday INRs may render adequate time for the patient to return to their usual, non-holiday habits, which would be similar to their pre-holiday INR. Nevertheless, as stated previously, there was great variability in the time from INR collection to the respective holidays, so these interpretations should be made cautiously.
While the INRs before and after Independence and Columbus Day had statistically significant differences, the post-holiday INR remained within goal range. In spite of that, both Independence and Columbus Day yielded INRs that were significantly increased to 2.81 and 2.82, respectively. These values are on the higher end of the most desired range of 2 - 3, and were the highest post-holiday INRs observed, compared to other holidays. Under the setting of unchanged warfarin doses, such significant fluctuations in INR were unexpected, thus denoting variations in diet, medications, or substance use that may have triggered, or would continue to cause, an uptrend in INR. An INR that continues to increase, and left unrecognized, could potentially reach supratherapeutic levels and toxic effects without early intervention and patient education [1].
With respect to drug interactions, the most common interacting medication was aspirin, which can increase the risk of bleeding through additive effects on hemostasis but is not known to have effects on INR. The second most common interacting medication was amiodarone, which can increase both the bleeding risk and INR due to amiodarone’s inhibition of cytochrome P450 2C9, thereby inhibiting the metabolism, increasing the plasma concentration, and enhancing the anticoagulation effect of warfarin [1]. Interacting anti-infectives included azithromycin, amoxicillin, and ketoconazole; diligent monitoring of INR is warranted to prevent supratherapeutic levels and adverse outcomes while on concurrent therapy. For temporary medications that inhibit the metabolism of warfarin, like anti-infectives, as opposed to with a chronic medication such as aspirin or amiodarone, the clinician must be conservative and anticipate a subsequent increase in INR (upon initiation of the interacting agent) and decrease in INR (upon discontinuation of the interacting agent) [1-2, 6].
There have been reports of increased bleeding in warfarin-users, even those with therapeutic INRs, and this may be potentially due to defects in the blood coagulation pathway [18]. Consequently, prudent monitoring of INR and signs/symptoms of bleeding is of chief concern, even in patients with INR in the target range. Due to issues separate from INR and anticoagulation, there have been reports of new hospital admissions, readmissions after discharge, and even death (such as cardiac mortality) around the time of holidays and sporting events [19-22]. These adverse outcomes may be attributed to lack of prompt evaluation and management, delays in timely follow-up care, and new or intensified activities or emotions related to such occasions. Special attention is required around the holiday season in patients on high-risk medications such as warfarin, and especially so in patients with risk factors, such as end-stage renal disease. The significantly higher risk of poor outcomes, such as major bleeding, stroke, and even mortality, has been well characterized in warfarin-users who are on hemodialysis/have end-stage renal disease; therefore, vigilant monitoring is imperative in this population, especially when they are most vulnerable to lifestyle changes, such as around the holidays [23-28].
Study limitations exist based on the retrospective design of the study, and assumptions were made that the electronic medical record reflected all potentially interacting drugs, changes in diet and medications, adherence patterns, and substance use. Further, this study assessed the impact of holidays over a short period in one center, and we acknowledge this as a shortcoming; thus, we recommend longer follow-up and collaboration with more participating centers to increase the sample size for future studies. Of note, this study was conducted prior to the COVID-19 pandemic and so all patients were being seen in person - inevitably, close monitoring remained a challenge, despite diligence in patient outreach. Most patients in this study were Caucasian, which is not generalizable to all ethnicities and their associated dietary customs around the holidays, which may have implications on INR. Lastly, the acceptable timing of INR collection was 2 weeks pre- and post-holiday; as such, there were a few overlapping INR values based on the proximity of holidays, such as Christmas and New Year’s. Ideally, the timeframe for the INR should be much closer to the actual holiday to prevent convergence of data.
In practice, clinicians should comprehensively capture concomitant drug/herbal usage through a thorough patient interview, prescription drug database, or contact with local pharmacies. Patients should be inquired about detailed holiday/travel plans to prevent any overlooked interactions that may have additive effects on INR. The vicinity of the INR draw can be made close to each holiday, perhaps by way of self-monitoring, telephone/remote monitoring, or drive-up methods [29-31]. Achieving therapeutic levels of INR in warfarin-users is indispensable in yielding favorable clinical outcomes, such as reducing rates of stroke, systemic embolism, bleeding, hospitalization, and mortality [1-2, 6]. We hope and anticipate that the results of this study would be hypothesis-generating and assist in the development of larger prospective studies.
Conclusion
Based on the results of our study, we found that there was a significant increase in INR before and after Independence Day and Columbus Day. There may be substantial changes in medication adherence and dietary patterns, which may impact the level of anticoagulation in warfarin-users. Future studies are needed to delineate the possible association of holidays on INR to optimize the care of patients on warfarin therapy.
Acknowledgments
The authors would like to thank the cardiology team at Loma Linda University Health for assistance with the research proposal and data extraction.
Financial Disclosure
This research received no external funding.
Conflict of Interest
The authors declare no conflict of interest.
Informed Consent
A waiver of informed consent was granted by the Institutional Review Board at Loma Linda University Health because this study was a retrospective chart review.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Rachel Ryu, Khaled Bahjri, and Huyentran Tran. The first draft of the manuscript was written by Rachel Ryu and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Data Availability
De-identified participant data, study methodology, and statistical analyses will be shared upon reasonable request by the corresponding author. Data will be shared electronically in a timely manner for a length of time justifiable for researchers whose purpose is to further explore and expand on this topic.
Abbreviations
INR: international normalized ratio; TTR: time-in-therapeutic range; US: United States
| References | ▴Top |
- Product Information: COUMADIN(R) oral tablets, warfarin sodium oral tablets. Bristol-Myers Squibb Company (per manufacturer), Princeton, NJ. 2019.
- Lane DA, Lip GY. Maintaining therapeutic anticoagulation: the importance of keeping "within range". Chest. 2007;131(5):1277-1279.
doi pubmed - Sevilla-Cazes J, Finkleman BS, Chen J, Brensinger CM, Epstein AE, Streiff MB, Kimmel SE. Association between patient-reported medication adherence and anticoagulation control. Am J Med. 2017;130(9):1092-1098.e1092.
doi pubmed - McAlister FA, Wiebe N, Hemmelgarn BR. Time in therapeutic range and stability over time for warfarin users in clinical practice: a retrospective cohort study using linked routinely collected health data in Alberta, Canada. BMJ Open. 2018;8(1):e016980.
doi pubmed - Ryu R, Tran R. DOACs in mechanical and bioprosthetic heart valves: a narrative review of emerging data and future directions. Clin Appl Thromb Hemost. 2022;28:10760296221103578.
doi pubmed - Hirsh J, Dalen J, Anderson DR, Poller L, Bussey H, Ansell J, Deykin D. Oral anticoagulants: mechanism of action, clinical effectiveness, and optimal therapeutic range. Chest. 2001;119(1 Suppl):8S-21S.
doi pubmed - Penning-van Beest FJ, Koerselman J, Herings RM. Risk of major bleeding during concomitant use of antibiotic drugs and coumarin anticoagulants. J Thromb Haemost. 2008;6(2):284-290.
doi pubmed - Manotti C, Quintavalla R, Pattacini C, Pini M. Seasonal variation of oral anticoagulant effect. Thromb Haemost. 1994;71(6):802-803.
doi pubmed - Salobir B, Sabovic M, Peternel P. Intensity of long-term treatment with warfarin is influenced by seasonal variations. Pathophysiol Haemost Thromb. 2002;32(4):151-154.
doi pubmed - Van Patot MC, Hill AE, Dingmann C, Gaul L, Fralick K, Christians U, Honigman B, et al. Risk of impaired coagulation in warfarin patients ascending to altitude (>2400 m). High Alt Med Biol. 2006;7(1):39-46.
doi pubmed - Federal Holidays and Research Room Closings. National Archives and Records Administration. Retrieved October 5, 2019, from https://www.archives.gov/news/federal-holidays.
- https://www.niaaa.nih.gov/alcohols-effects-health/overview-alcohol-consumption/what-standard-drink#:∼:text=In%20the%20United%20States%2C%20one,which%20is%20about%2040%25%20alcohol.
- U.S. holiday travel. Bureau of Transportation Statistics. (n.d.). Retrieved October 10, 2019, from https://www.bts.gov/archive/publications/america_on_the_go/us_holiday_travel/entire.
- Independence Day. GovInfo. (May 18, 2022). Retrieved November 5, 2022, from https://www.govinfo.gov/features/independence-day.
- "These Are America's Favorite 4th of July Foods, According to Food Network." (June 18, 2019). TodayShow. Retrieved October 5, 2019, from, https://www.today.com/food/food-network-poll-reveals-americans-favorite-4th-july-foods-t156609.
- Columbus Day, 2018. Proclamation 9801 of October 5, 2018. The Federal Register. 83 FR 51615. October 24, 2018, from https://www.federalregister.gov/documents/2018/10/11/2018-22335/columbus-day-2018.
- Eat like a sailor to celebrate Columbus Day. October 5, 2012. The daily meal. Retrieved October 24, 2018, from https://www.thedailymeal.com/eat-sailor-celebrate-columbus-day.
- Dargaud Y, Hoffman M, Lefrapper L, Lin FC, Genty A, Chatard B, Marin S, et al. Bleeding risk in warfarinized patients with a therapeutic international normalized ratio: the effect of low factor IX levels. J Thromb Haemost. 2013;11(6):1043-1052.
doi pubmed - Lapointe-Shaw L, Austin PC, Ivers NM, Luo J, Redelmeier DA, Bell CM. Death and readmissions after hospital discharge during the December holiday period: cohort study. BMJ. 2018;363:k4481.
doi pubmed - Mohammad MA, Karlsson S, Haddad J, Cederberg B, Jernberg T, Lindahl B, Frobert O, et al. Christmas, national holidays, sport events, and time factors as triggers of acute myocardial infarction: SWEDEHEART observational study 1998-2013. BMJ. 2018;363:k4811.
doi pubmed - Phillips DP, Jarvinen JR, Abramson IS, Phillips RR. Cardiac mortality is higher around Christmas and New Year's than at any other time: the holidays as a risk factor for death. Circulation. 2004;110(25):3781-3788.
doi pubmed - Hung DP, Lin SM, Liu PP, Su IM, Hsu JY, Wu TY, Lin CC, et al. Evaluating the "holiday season effect" of hospital care on the risk of mortality from pulmonary embolism: a nationwide analysis in Taiwan. Sci Rep. 2021;11(1):19376.
doi pubmed - Tsai C, Marcus LQ, Patel P, Battistella M. Warfarin use in hemodialysis patients with atrial fibrillation: a systematic review of stroke and bleeding outcomes. Can J Kidney Health Dis. 2017;4:2054358117735532.
doi pubmed - Liu G, Long M, Hu X, Hu CH, Liao XX, Du ZM, Dong YG. Effectiveness and safety of warfarin in dialysis patients with atrial fibrillation: a meta-analysis of observational studies. Medicine (Baltimore). 2015;94(50):e2233.
doi pubmed - Tan J, Liu S, Segal JB, Alexander GC, McAdams-DeMarco M. Warfarin use and stroke, bleeding and mortality risk in patients with end stage renal disease and atrial fibrillation: a systematic review and meta-analysis. BMC Nephrol. 2016;17(1):157.
doi pubmed - Dahal K, Kunwar S, Rijal J, Schulman P, Lee J. Stroke, major bleeding, and mortality outcomes in warfarin users with atrial fibrillation and chronic kidney disease: a meta-analysis of observational studies. Chest. 2016;149(4):951-959.
doi pubmed - Chan KE, Lazarus JM, Thadhani R, Hakim RM. Anticoagulant and antiplatelet usage associates with mortality among hemodialysis patients. J Am Soc Nephrol. 2009;20(4):872-881.
doi pubmed - Randhawa MS, Vishwanath R, Rai MP, Wang L, Randhawa AK, Abela G, Dhar G. Association Between Use of Warfarin for Atrial Fibrillation and Outcomes Among Patients With End-Stage Renal Disease: A Systematic Review and Meta-analysis. JAMA Netw Open. 2020;3(4):e202175.
doi pubmed - Wittkowsky AK, Nutescu EA, Blackburn J, Mullins J, Hardman J, Mitchell J, Vats V. Outcomes of oral anticoagulant therapy managed by telephone vs in-office visits in an anticoagulation clinic setting. Chest. 2006;130(5):1385-1389.
doi pubmed - Zobeck B, Carson E, MacDowell M, Hunt A, Reeder A. Appointment attendance and patient perception of drive-up INR testing in a rural anticoagulation clinic during the COVID-19 pandemic. J Am Coll Clin Pharm. 2021;4(4):459-464.
doi pubmed - Heneghan C, Ward A, Perera R, Self-Monitoring Trialist C, Bankhead C, Fuller A, Stevens R, et al. Self-monitoring of oral anticoagulation: systematic review and meta-analysis of individual patient data. Lancet. 2012;379(9813):322-334.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.