

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 13, Number 5, October 2022, pages 283-288

Burnout of Support Personnel in the Cardiac Catheterization Laboratory
Jacob Alexa, d ![]() , Hashil Patelb, Marc T. Zughaiba, Ankita Aggarwalb, Anudeep Komminenia, Maja Pietrowiczc, Marcel Zughaibb
, Hashil Patelb, Marc T. Zughaiba, Ankita Aggarwalb, Anudeep Komminenia, Maja Pietrowiczc, Marcel Zughaibb
aDepartment of Internal Medicine, Michigan State University/Ascension Providence Hospital, Southfield, MI, USA
bDepartment of Cardiology, Michigan State University/Ascension Providence Hospital, Southfield, MI, USA
cMichigan State University, East Lansing, MI, USA
dCorresponding Author: Jacob Alex, Department of Internal Medicine, Michigan State University/Ascension Providence Hospital, Southfield, MI, USA
Manuscript submitted September 26, 2022, accepted October 11, 2022, published online October 25, 2022
Short title: Burnout of Support Personnel in the CCL
doi: https://doi.org/10.14740/cr1439
| Abstract | ▴Top |
Background: Healthcare professionals experience stressors in the workplace, putting them at elevated risk for burnout. The cardiac catheterization lab is a dynamic environment with high-acuity patients; however, little has been published investigating burnout syndrome among healthcare workers. The aim of the study was to identify the prevalence, demographic, and workload factors, which contribute to burnout syndrome among this population.
Methods: This is a multicenter cross-sectional study assessing burnout with the Maslach Burnout Inventory (MBI) among registered nurses and registered cardiac invasive specialists working in the catheterization/electrophysiology lab and cardiac observation unit at four hospital centers in the metro Detroit area.
Results: Of the 48 participants, 69% (n = 33) were female. The overall prevalence of burnout syndrome was 33% (n = 16). Significantly more males experienced burnout than females (P < 0.05). Of the participants experiencing burnout, a greater proportion worked in the catheterization lab compared to the cardiac observation unit (93.8% vs. 6.3%). Burned-out participants worked on average more day shifts, ST-segment elevation myocardial infarction (STEMI) call shifts, and extended day shifts per month compared to those not experiencing burnout. The rate of burnout was significantly higher for individuals reporting increased stress during the pandemic (69% vs. 18%, P < 0.05).
Conclusions: Registered nurses and registered cardiac invasive specialists working in the cardiac catheterization or electrophysiology lab experience elevated levels of burnout. Greater attention should be placed in identifying and optimizing workplace variables which contribute to burnout among this population.
Keywords: Burnout; Cardiac catheterization; Nurse; Maslach Burnout Inventory
| Introduction | ▴Top |
With the advent of the first coronary artery angioplasty in 1977, the cardiac catheterization lab (CCL) has become the center stage for reducing mortality in patients with ST-segment elevation myocardial infarction (STEMI) [1]. Since its inception, utilization of the CCL has expanded to a multitude of complex percutaneous interventions involving multidisciplinary teams [2, 3]. Healthcare workers functioning within this environment expose themselves to unique stressors due to the high acuity of patients, dynamic work environments with changing schedules, rapidly changing technology, and sleep deprivation. Registered nurses (RNs) and registered cardiovascular invasive specialists (RCISs) function in multiple roles within the CCL. While working alongside physician operators, their duties involve providing patient care, pre-, intra-, and post procedures, assisting during procedures, and operating all diagnostic and therapeutic equipment [4]. Caring for the patients in CCL requires high aptitude while also maintaining empathy, putting RNs and RCIS at higher risk of experiencing burnout.
The implications of burnout are far-reaching, affecting patients, healthcare workers, and the healthcare system as a whole. Burnout is associated with increased cognitive impairment and adverse patient events, including increased rates of healthcare-associated infections and self-reported errors [5-8]. Increased rates of hypertension, myocardial infarction, substance abuse, depression, and anxiety are observed in healthcare professionals experiencing burnout [9]. Hospital systems can experience increased workplace conflict, distrust of administration, and absenteeism leading to worsening staffing shortages [10-12].
The World Health Organization now defines the psychological syndrome of burnout in the International Classification of Diseases, 11th Revision (ICD-11) as exhaustion, detachment, and reduced efficacy resulting from mismanagement of chronic workplace stress [13]. The seminal work describing burnout was done by Maslach et al, who developed the Maslach Burnout Inventory (MBI), a survey taking into account three components: emotional exhaustion, depersonalization, and reduced personal accomplishment [14]. Emotional burnout is characterized by psychosomatic symptoms, including headaches, sleepiness, fatigue, and anhedonia. Depersonalization manifests as increased cynicism and reduced interpersonal contact with patients. Decreased sense of personal accomplishment can lead to a feeling of incompetence and a propensity to evaluate oneself negatively.
Burnout syndrome has been well described in the literature in many healthcare environments, including the emergency department (ED), operating room, and critical care units. There is a gap in the literature investigating burnout syndrome among healthcare workers in the CCL. Our study aims to evaluate the prevalence of burnout syndrome among RNs and RCIS involved in the care of patients in the CCL, electrophysiology lab (EPL), and cardiac observation unit (COU).
| Materials and Methods | ▴Top |
A cross-sectional survey of 48 full-time RNs and RCISs was performed at three tertiary care centers in the southeast Michigan region. Approval was obtained from the institutional review board (IRB) of respective hospitals. The STROBE reporting guidelines were used to present this study. The data were collected from May 11, 2021, to August 30, 2021. The CCL/EPL and COU staff were approached during their shifts and invited to participate in the study. They were given a brief overview of the study. After obtaining their informed consent to participate, they were emailed a link to complete the electronic survey.
An electronic version of the Maslach Burnout Inventory for Human Services Survey (MBI) was administered to the participating CCL and COU staff. The MBI is a validated 22-item survey that considers three components: emotional exhaustion, depersonalization, and reduced personal accomplishment. The MBI employs a Likert scale with responses ranging from 0 to 6 (0 = never, 1 = a few times a year, 2 = once a month or less, 3 = a few times a month, 4 = once a week, 5 = a few times a week, 6 = every day). Corresponding demographic characteristics were collected in a separate section of the survey. Responses were collected on the Google Workplace Sheets application; no personal identifying information was collected. Previously established cutoffs included the following, emotional exhaustion (scores of 27 or higher), depersonalization (scores of 10 or higher), and personal accomplishment (scores lower than 33) [15, 16]. Burnout was defined as anyone that met the critical value for emotional exhaustion and/or depersonalization [16, 17].
Continuous variables are expressed as mean ± standard deviation (SD) and categorical variables as absolute numbers and percentages. Continuous variables were tested with Student’s t-test. Fisher’s exact test was used to assess differences in categorical variables. Statistical analysis was performed using GraphPad Prism 8 (GraphPad Software, San Diego, California). Statistical significance was defined as a two-tailed P value ≤ 0.05.
This study has been approved by the IRB at Ascension Providence Hospital in Southfield and Novi, MI, Ascension Providence Rochester Hospital, in Rochester, MI, Ascension St. John Hospital in Detroit, MI (IRB study #1731690-4). This study was deemed ethically compliant from the IRB.
| Results | ▴Top |
We received completed surveys from 48 of 87 staff members, with a response rate of 55%. Out of all the respondents, 15 (31.3%) were males, and 33 (68.8%) were females (Table 1). There were five respondents aged 18 to 29, 17 aged 30 to 39, 10 aged 40 to 49, 13 aged 50 to 59, and three older than 60 years of age.
 Click to view | Table 1. Demographic Information for Overall Population (N = 48) |
Thirty-four (70.8%) of the respondents worked in the interventional lab, five (10.4%) in the EPL, and nine (18.8%) in the COU (Table 2). The distribution of experience levels is described in Table 2. Twenty-three (48%) respondents had less than 5 years of work experience. The average number of day shifts (defined as a scheduled shift ranging from 9 to 12 h) each respondent works per month was 16.4 ± 4. The average number of extended shifts (defined as any shift beyond scheduled hours) each respondent works per month was 2.5 ± 2.5. The number of STEMI calls (defined as a 24-h shift starting at 7 am) each respondent works per month was 7.2 ± 3.4.
Click to view | Table 2. Work-Related Demographic Information for Overall Population |
The average emotional exhaustion score for the respondents was 18.81 ± 12 (a higher score indicates a higher level of burnout) (Table 3). Fourteen respondents (29.17%) had emotional exhaustion scores above the critical value of 27, indicating burnout. The average depersonalization score was 3.77 ± 3.74 (a higher score indicating higher level of burnout). Seven respondents (14.58%) had depersonalization scores above the critical value of 10, indicating burnout. The average personal accomplishment score was 34.38 ± 10.05; however, we did not include this component in our criteria for burnout.
Click to view | Table 3. Burnout Scores for Overall Population |
The overall prevalence of burnout syndrome was 33.3% (16 respondents). Higher burnout was seen in males; 60% of males compared to 21% of females (P < 0.05) met burnout criteria (Fig. 1a). A respondent working in the COU has a 29% chance of experiencing burnout as a respondent working in the CCL/EPL (P = 0.24, 95% confidence interval (CI): 0.05 to 1.24). While it did not meet statistical significance, the study sample size was not powered to detect the difference. Higher rates of burnout were seen in participants who worked on average more day shifts, STEMI call shifts, and extended day shifts per month than non-burned-out participants; however, this trend was not statistically significant (Fig. 1b). The burnout rate is significantly higher for individuals reporting increased stress during the pandemic versus those who did not report increased stress (68.75% vs. 17.86%, P < 0.05).
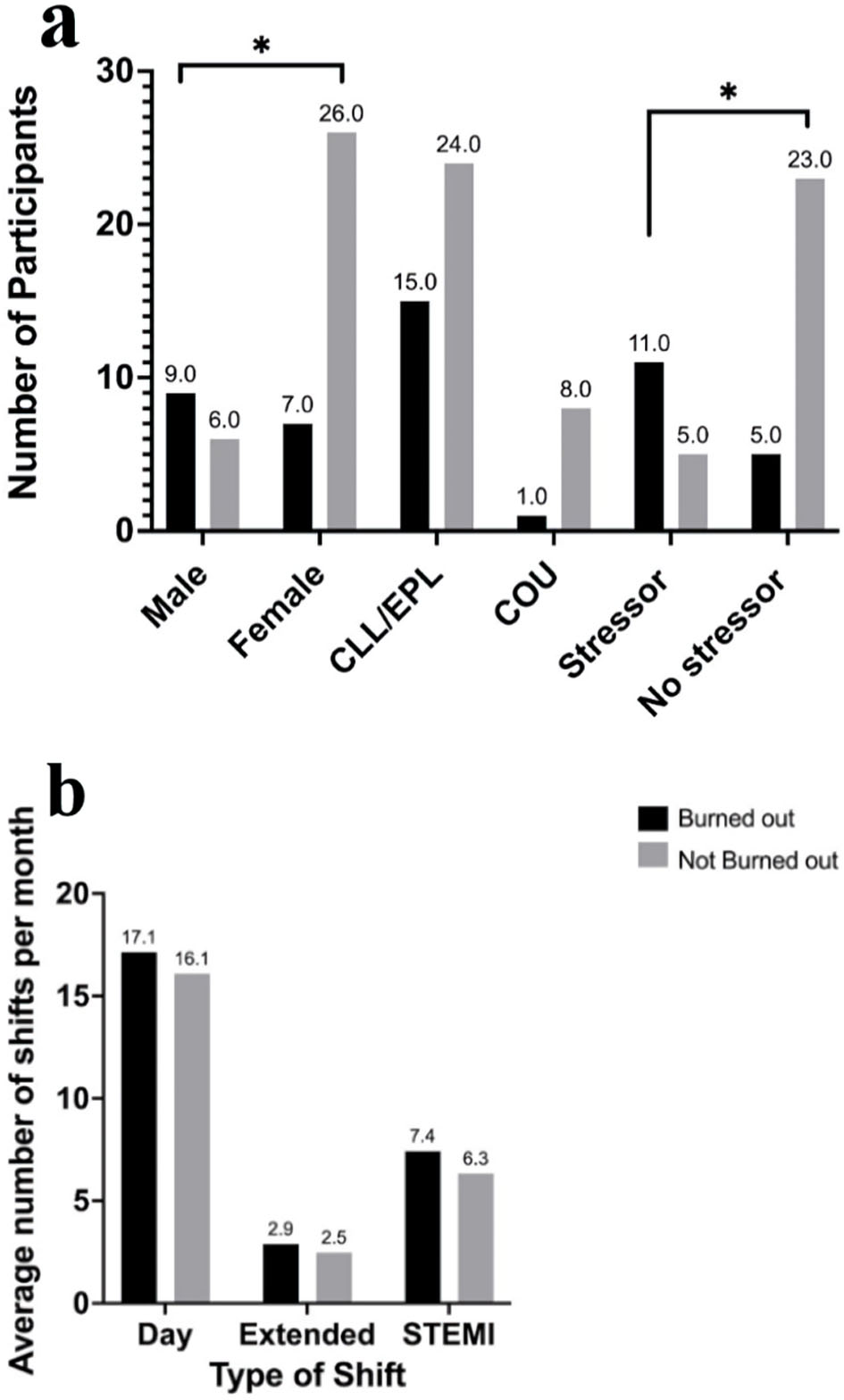 Click for large image | Figure 1. (a) Number of participants indicated above each bar who are burned out and not burned out, in each category listed along the x axis. *P value < 0.05. (b) Number and type of shifts completed by burned-out and not burned-out individuals, with the average number indicated above each bar. CCL: catheterization lab; EPL: electrophysiology lab; COU: cardiac observation unit; STEMI: ST-segment elevation myocardial infarction. |
| Discussion | ▴Top |
Burnout affects healthcare workers in all roles and settings. The prevalence of burnout varies among different departments in the hospital and has been well documented in most hospital settings [18-20]. In our study, the prevalence of burnout in the CCL/EPL was found to be 38.5%. A review of 17 studies found that as many as 26% of ED nurses reported some effects of burnout, with even higher rates reported among operating room staff at 82.6% [21, 22]. There is a large amount of variability between studies reporting burnout within the same department; reported burnout in adult critical nurses ranges from 16% to 81% [22, 23]. Some of the variability can be attributed to studies applying a diverse range of measurement tools. The MBI was used in our study. There remains a paucity of data on burnout in the CCL. To get a better understanding of the true CLL burnout rate, measurements may need to be repeated at different hospital systems with the use of one “gold standard” burnout assessment tool.
Burnout has been more critical than ever since the beginning of 2020, when the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) started spreading worldwide, causing the coronavirus disease 2019 (COVID-19) pandemic. Healthcare workers were called to care for patients stricken by this disease, expected to work longer hours in different environments, wear personal protective equipment (PPE), and care for high-acuity patients while at the same time exposing themselves to the virus. In one study with 1,795 respondents, 40.3% of healthcare workers, particularly nurses (45%) and physicians (31%) experienced burnout during the pandemic [24]. A study looking at 1,153 Italian healthcare professionals during the pandemic found that at least one-third were experiencing a component of burnout [25]. In our study, individuals who reported increased stress during the pandemic had significantly higher rates of burnout than those who did not report increased stress (68.75% vs. 17.86%, P < 0.05). Our respondents were unlikely to be involved in the care of COVID-9 patients; however, our findings suggest pandemic-related factors within or outside the hospital contributed to them experiencing burnout. Fear of contacting SARS-CoV-2, increased PPE use, vaccine mandates, employment uncertainties, and pandemic-related stressors at home likely contributed to developing burnout.
The modern CCL looks drastically different from its inception, where it was primarily used for diagnostic evaluation of the coronary arteries before cardiac surgery. Today the CCL offers a wide range of catheter-based therapies, including complex coronary, peripheral endovascular, and structural heart interventions [2, 3]. As newer interventions are developed, CCLs around the country move to rapidly adopt the latest minimally invasive procedures, all while emphasizing same-day discharge [2, 3]. A significant proportion of the time spent by the RNs and RCISs in the CCLs involves operating hemodynamic monitoring systems and the use of electronic medical records (EMRs). EMR usage has been associated with an increased prevalence of burnout [26]. It can be postulated that the heavy usage of EMRs by CCLs staff may take away from interpersonal interactions and direct patient care, which may be a driver for burnout.
Our data did show a trend of burned-out staff doing more day, extended, and STEMI call shifts on average compared to non-burned-out staff, but this did not reach statistical significance. However, our study may be underpowered to show a difference. Similar results were seen by Barbosa et al, whose study of 67 on-call physicians showed no significant correlation between weekly on-call hours and any of the three dimensions of burnout syndrome [27]. In contrast, Balch et al published a larger study of 7,900 surgeons that showed burnout exhibited a threshold effect at ≥ 2 nights on call/week (≤ 1 night on call/week, 30%; ≥ 2 nights on call/week, 44% to 46%) [28]. When comparing our study to those published by Barbosa et al [27] and Balch et al [28], one may suggest that by increasing the number of participants, we may see statistically significant increased burnout in staff doing more day, extended, and STEMI on-call shifts. The number of shifts done is only one variable affecting burnout; workload has a greater impact on burnout [29]. Data from neonatal intensive care unit (NICU) nurses demonstrated higher burnout in centers with higher volume and higher admission rates [26]. Modern CCLs are designed to maximize caseloads, which may have deleterious effects on staff, as more intellectual effort is needed to take on more cases and greater emotional effort to talk to patients and their families. Future studies investigating the relationship between burnout and CLL caseloads could provide valuable insight into developing optimal workloads to maximize efficacy while deterring burnout.
Our study showed higher burnout among staff in the CCL/EPL than in the COU, 38.5% versus 12.5%, (P = 0.24) (Fig. 1a). We suspect the lack of statistical significance was due to having only nine respondents from the COU compared to 39 respondents from the CCL/EPL. We decided to compare burnout between these two environments because they both provide care for the same patient at different courses of their treatment. It is important to note that at the studied hospitals, although the CCL/EPL and COU are in close physical proximity, the staff exclusively work in either department and have different duties and work hours. The CCL/EPL RNs and RCIS are expected to maintain proficiency when assisting with the latest procedure and ensure patient safety from admission to discharge or transfer. The pre-/intra-/post-procedure care involves performing patient assessments, administering medications, monitoring and recording electrocardiograms and hemodynamic data, operating mechanical assist devices, stocking supplies, and performing efficient patient turnover [4]. The COU RNs manage either pre- or post-procedure patients; their duties are more typical of post-anesthesia care unit (PACU) nurses. COU RNs monitor patient vitals, check their level of consciousness, monitor for post-catheterization complications, administer medications, and communicate with patients’ family members. With current consensus guidelines supporting door-to-balloon time in 90 min or less in patients with STEMI [30], it is a race against time for CCL staff to arrive on-site and complete coronary reperfusion. If STEMI patients are not reperfused in time, they are at risk of going into cardiogenic shock; large center CCLs often deploy mechanical assist devices. These patients are at high risk of decompensating, and CCL staff are expected to perform resuscitative measures immediately. This stark difference in the level of urgency and acuity in patients between the CCL/EPL and COU could explain the higher burnout seen in CCL/EPL staff. Health care workers in high acuity and procedure dominant departments like the operating room and critical care units experience higher rates of burnout [21, 22].
A major limitation of this study is a low response rate at 55%. Survey fatigue is a major contributing factor, as hospital employees are frequently subjected numerous workplace related surveys. There may also be a selection bias, where burned-out individuals may be less inclined to participate in a voluntary survey. Another limitation is recruitment of participants from the same geographical area in southeast Michigan and smaller sample size. CCLs generally operate with smaller number of staff compared to other hospital units, as such numerous CCLs would have to be recruited for a higher-powered study. This pilot study highlights burnout among the at-risk population of healthcare care workers in the CCL, which had not previously been investigated.
A follow-up study with larger national recruitment would be needed to have more generalizable results.
This pilot study shows that assessment of burnout in the CCL can be quantified with the reliable and validated MBI. Burnout among the at-risk population of healthcare care workers in the CCL has not previously been investigated. The MBI can be deployed in the CCLs across the country to identify staff members that are particularly at risk. It adds to a large body of research that burnout has a high prevalence in high-stress departments within the health care system. Quality in the CCL is often defined as performing the correct procedure, on an ideal candidate, at the appropriate time [31]. However, to ensure the delivery of quality care, CCL staff must ensure their mental wellbeing, as failure to do so has negative implications for patients and hospital organizations. The CCLs could provide better care for patients by implementing organizational changes which reduce burnout among health care workers.
Learning points
Burnout is highly prevalent among RNs and registered cardiac invasive specialists working in the CCL.
The MBI can be utilized to effectively quantify burnout in the CCL.
Participants reporting higher pandemic stress were significantly more burned out compared to those not reporting higher pandemic stress.
Acknowledgments
We would like to thank Jack Cain for participant recruitment and all catheterization lab staff for their participation, and thanks to Nancy Jackson for statistical support and study design.
Financial Disclosure
Funding was provided by Ascension Providence Hospital Department of Graduate Medical Education.
Conflict of Interest
No conflict of interest to declare.
Informed Consent
Informed consent was received from all participants.
Author Contributions
Jacob Alex and Hashil Patel contributed to literature review, developed protocol, and wrote manuscript. Marc T. Zughaib: statistical support, data collection, and review of manuscript. Ankita Aggarwal, Anudeep Kommineni, and Maja Pietrowicz contributed to data collection and reviewed manuscript. Marcel Zughaib: protocol design and review of manuscript.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
| References | ▴Top |
- Karam N, Bataille S, Marijon E, Tafflet M, Benamer H, Caussin C, Garot P, et al. Incidence, mortality, and outcome-predictors of sudden cardiac arrest complicating myocardial infarction prior to hospital admission. Circ Cardiovasc Interv. 2019;12(1):e007081.
doi pubmed - Foot DK, Lewis RP, Pearson TA, Beller GA. Demographics and cardiology, 1950-2050. J Am Coll Cardiol. 2000;35(4):1067-1081.
doi - Maier W, Camici P, Windecker S, Pfiffner D, Wijns W, Meier B, Working Group Coronary Circulation of the European Society of Cardiology. The European Registry of Cardiac Catheter Interventions 1997. Eur Heart J. 2002;23(24):1903-1907.
doi pubmed - Amoroso G, Sarti M, Bellucci R, Puma FL, D'Alessandro S, Limbruno U, Canova A, et al. Clinical and procedural predictors of nurse workload during and after invasive coronary procedures: the potential benefit of a systematic radial access. Eur J Cardiovasc Nurs. 2005;4(3):234-241.
doi pubmed - Arora M, Asha S, Chinnappa J, Diwan AD. Review article: burnout in emergency medicine physicians. Emerg Med Australas. 2013;25(6):491-495.
doi pubmed - Shanafelt TD, Balch CM, Bechamps G, Russell T, Dyrbye L, Satele D, Collicott P, et al. Burnout and medical errors among American surgeons. Ann Surg. 2010;251(6):995-1000.
doi pubmed - Cimiotti JP, Aiken LH, Sloane DM, Wu ES. Nurse staffing, burnout, and health care-associated infection. Am J Infect Control. 2012;40(6):486-490.
doi pubmed - Deligkaris P, Panagopoulou E, Montgomery A, Masoura E. Job burnout and cognitive functioning: A systematic review. Work and Stress. 2014;28:107-123.
doi - Salvagioni DAJ, Melanda FN, Mesas AE, Gonzalez AD, Gabani FL, Andrade SM. Physical, psychological and occupational consequences of job burnout: A systematic review of prospective studies. PLoS One. 2017;12(10):e0185781.
doi pubmed - Dyrbye LN, Shanafelt TD, Johnson PO, Johnson LA, Satele D, West CP. A cross-sectional study exploring the relationship between burnout, absenteeism, and job performance among American nurses. BMC Nurs. 2019;18:57.
doi pubmed - Leiter MP, Spence Laschinger HK. Relationships of work and practice environment to professional burnout: testing a causal model. Nurs Res. 2006;55(2):137-146.
doi pubmed - Jourdain G, Chenevert D. Job demands-resources, burnout and intention to leave the nursing profession: a questionnaire survey. Int J Nurs Stud. 2010;47(6):709-722.
doi pubmed - ICD-11 for mortality and morbidity statistics. https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/129180281. Accessed January 12, 2022.
- Maslach C, Jackson SE, Leiter MP. Maslach burnout inventory, third edition. In: Evaluating Stress: A Book of Resources. Lanham, MD, US: Scarecrow Education; 1997:191-218.
- Maslach C, Jackson S, Leiter MP. Maslach burnout inventory manual. Palo Alto: California Consulting Psychological Press Inc. 1996.
- Maslach C. Burnout: the cost of caring Cambridge. MA: ISHK. 2003.
- Prins JT, Gazendam-Donofrio SM, Tubben BJ, van der Heijden FM, van de Wiel HB, Hoekstra-Weebers JE. Burnout in medical residents: a review. Med Educ. 2007;41(8):788-800.
doi pubmed - Howlett M, Doody K, Murray J, LeBlanc-Duchin D, Fraser J, Atkinson PR. Burnout in emergency department healthcare professionals is associated with coping style: a cross-sectional survey. Emerg Med J. 2015;32(9):722-727.
doi pubmed - Chernoff P, Adedokun C, O'Sullivan I, McManus J, Payne A. Burnout in the emergency department hospital staff at Cork University Hospital. Ir J Med Sci. 2019;188(2):667-674.
doi pubmed - Tawfik DS, Phibbs CS, Sexton JB, Kan P, Sharek PJ, Nisbet CC, Rigdon J, et al. Factors associated with provider burnout in the NICU. Pediatrics. 2017;139(5):e20164134.
doi pubmed - Adriaenssens J, De Gucht V, Maes S. Determinants and prevalence of burnout in emergency nurses: a systematic review of 25 years of research. Int J Nurs Stud. 2015;52(2):649-661.
doi pubmed - Mealer M, Burnham EL, Goode CJ, Rothbaum B, Moss M. The prevalence and impact of post traumatic stress disorder and burnout syndrome in nurses. Depress Anxiety. 2009;26(12):1118-1126.
doi pubmed - Zhang XC, Huang DS, Guan P, SUBLIN Study Team. Job burnout among critical care nurses from 14 adult intensive care units in Northeastern China: a cross-sectional survey. BMJ Open. 2014;4(6):e004813.
doi pubmed - Sung CW, Chen CH, Fan CY, et al. Burnout in medical staffs during a coronavirus disease (COVID-19) pandemic. Rochester, NY: Social Science Research Network; 2020. https://papers.ssrn.com/abstract=3594567. Accessed January 12, 2022.10.2139/ssrn.3594567
- Barello S, Palamenghi L, Graffigna G. Burnout and somatic symptoms among frontline healthcare professionals at the peak of the Italian COVID-19 pandemic. Psychiatry Res. 2020;290:113129.
doi pubmed - Profit J, Sharek PJ, Amspoker AB, Kowalkowski MA, Nisbet CC, Thomas EJ, Chadwick WA, et al. Burnout in the NICU setting and its relation to safety culture. BMJ Qual Saf. 2014;23(10):806-813.
doi pubmed - Barbosa FT, Leao BA, Tavares GM, Santos JG. Burnout syndrome and weekly workload of on-call physicians: cross-sectional study. Sao Paulo Med J. 2012;130(5):282-288.
doi pubmed - Balch CM, Shanafelt TD, Dyrbye L, Sloan JA, Russell TR, Bechamps GJ, Freischlag JA. Surgeon distress as calibrated by hours worked and nights on call. J Am Coll Surg. 2010;211(5):609-619.
doi pubmed - Weigl M, Stab N, Herms I, Angerer P, Hacker W, Glaser J. The associations of supervisor support and work overload with burnout and depression: a cross-sectional study in two nursing settings. J Adv Nurs. 2016;72(8):1774-1788.
doi pubmed - Nathan AS, Raman S, Yang N, Painter I, Khatana SAM, Dayoub EJ, Herrmann HC, et al. Association between 90-minute door-to-balloon time, selective exclusion of myocardial infarction cases, and access site choice: insights from the Cardiac Care Outcomes Assessment Program (COAP) in Washington State. Circ Cardiovasc Interv. 2020;13(9):e009179.
doi pubmed - Henien S, Aronow HD, Abbott JD. Quality management in the cardiac catheterization laboratory. J Thorac Dis. 2020;12(4):1695-1705.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.