

| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Original Article
Volume 11, Number 6, December 2020, pages 405-411
Relationship Between Kihon Checklist Score and Anxiety Levels in Elderly Patients Undergoing Early Phase II Cardiac Rehabilitation
Akio Honzawaa, Miho Nishitani-Yokoyamaa, b, h, Kazunori Shimadaa, b, c, Mitsuhiro Kunimotob, Miki Yamadaa, Tomomi Matsubarab, Rie Matsumorib, Kei Fujiwarab, Abidan Abulimitib, c, Tatsuro Aikawab, Shohei Ouchib, Megumi Shimizub, Yurina Sugitab, Akie Shimadad, Taira Yamamotod, Atsushi Amanod, Tohru Asaid, Masakazu Saitoe, Tomoyuki Morisawae, Tetsuya Takahashie, Toshiyuki Fujiwarae, f, Hiroyuki Daidac, e, Tohru Minaminob, g
aCardiovascular Rehabilitation and Fitness, Juntendo University Hospital, Tokyo, Japan
bDepartment of Cardiovascular Biology and Medicine, Juntendo University Graduate School of Medicine, Tokyo, Japan
cSpotology Center, Juntendo University Graduate School of Medicine, Tokyo, Japan
dDepartment of Cardiovascular Surgery, Juntendo University Graduate School of Medicine, Tokyo, Japan
eJuntendo University, Faculty of Health Science, Tokyo, Japan
fDepartment of Rehabilitation Medicine, Juntendo University Graduate School of Medicine, Tokyo, Japan
gJapan Agency for Medical Research and Development-Core Research for Evolutionary Medical Science and Technology (AMED-CREST), Japan Agency for Medical Research and Development, Tokyo, Japan
hCorresponding Author: Miho Nishitani-Yokoyama, Department of Cardiovascular Biology and Medicine, Juntendo University Graduate School of Medicine, 2-1-1 Hongo, Bunkyo-ku, Tokyo 113-8421, Japan
Manuscript submitted September 15, 2020, accepted September 22, 2020, published online November 2, 2020
Short title: Relationship Between Frailty Score and Anxiety
doi: https://doi.org/10.14740/cr1165
| Abstract | ▴Top |
Background: The frailty state consists of not only physical but also psycho-emotional problems, such as cognitive dysfunction and depression as well as social problems. However, few reports have examined the relationship between frailty and anxiety levels in elderly patients undergoing cardiac rehabilitation (CR).
Methods: We analyzed 255 patients (mean age: 74.9 ± 5.8 years, 67% male) who participated in early phase II CR at Juntendo University Hospital. At the beginning of CR, patients carried out self-assessments based on the Kihon Checklist (KCL) and the State Trait Anxiety Inventory Form (STAI). Patients were divided into three groups: frailty group (n = 99, 39%), pre-frailty group (n = 81, 32%), and non-frailty group (n = 75, 29%) according to the KCL. We assessed results from the KCL scores and its relationship with anxiety levels.
Results: Among the three groups, there were no significant differences in age, underlying illnesses, or the prevalence of coronary risk factors. Depressive mood domains of the KCL were significantly higher in the frailty and pre-frailty groups than in the non-frailty groups (3.0 ± 1.5 vs. 1.4 ± 1.2 vs. 0.4 ± 0.6; P < 0.01). The state anxiety level was significantly higher in the frailty group than in the non-frailty group (41.6 ± 0.9 vs. 34.9 ± 1.0; P < 0.01). The trait anxiety levels were significantly higher in the frailty group and pre-frailty group than in the non-frailty group (45.5 ± 0.9 vs. 39.2 ± 1.0 vs. 35.1 ± 1.1; P < 0.01). State anxiety and trait anxiety also showed a significantly positive correlations with the KCL scores (r = 0.32 vs. 0.41, P < 0.01).
Conclusions: Frailty scores were positively correlated not only with physical function but also with depression mood and anxiety levels in elderly patients undergoing early phase II CR. These results suggest that assessment of depressive mood and anxiety is also important in elderly patients undergoing early phase II CR.
Keywords: Frailty; Anxiety; Elderly patients; Cardiac rehabilitation; Kihon Checklist
| Introduction | ▴Top |
As Japan’s population gradually becomes a “super-aged society”, the number of elderly patients with cardiovascular disease (CVD) has continued to increase [1]. Interestingly, frailty is an important prognostic factor in patients with CVD [2, 3]. Frailty is regarded as a geriatric syndrome associated with high vulnerability to stressors toward adverse health outcomes, resulting from the decreased reserves of multiple physiological systems [4]. Frailty is clinically considered to be an early form of physical, social or psychological disability. Therefore, functions of the elderly people should be assessed across multiple domains to identify frail individuals [5]. The Kihon Checklist (KCL), a self-administered questionnaire, is considered to be a useful tool for frailty screening in older adult populations [6]. Indeed, total KCL scores have been shown to correlate significantly with Fried’s frailty phenotype values [7].
Patients with CVD have a high rate of concurrent psycho-emotional stress [8], including depression and anxiety symptoms. It is noteworthy that approximately 20% of patients with ischemic heart disease and 25% of patients with heart failure experience psycho-emotional stress [9, 10]. Moreover, psycho-emotional stress is a risk factor for CVD and is associated with recurrence of CVD, re-hospitalization due to heart failure as well as mortality [11, 12]. Despite the impact of psycho-emotional stress on CVD, few reports have examined the relationship between frailty and anxiety levels in elderly patients with CVD. In the present study, we retrospectively examined the relationship between KCL score and anxiety levels in elderly patients undergoing early phase II cardiac rehabilitation (CR) at Juntendo University Hospital.
| Materials and Methods | ▴Top |
Study population
This was a retrospective cross-sectional study. We enrolled 658 consecutive patients who participated in early phase II CR program from November 2015 to December 2016 at Juntendo University Hospital, Tokyo, Japan. In Japan, the indications for CR in CVD patients include acute myocardial infarction, angina pectoris after open heart surgery, chronic heart failure, major vessel disease, peripheral artery disease and post-transcatheter aortic valve implantation [13]. CR comprises medical evaluation of patients, exercise therapy, education for secondary prevention and support of psychosocial factors [14]. The present study enrolled elderly patients (aged ≥ 65 years) who participated in CR and were evaluated for clinical parameters, including risk profiles and physical function. Of the initial 658 patients we enrolled, 233 patients were excluded for being aged < 65 years and 170 patients lacked anxiety evaluation scores. This resulted in 255 patients being included in the study who met all criteria. The purpose of the study was explained in writing to the patients and consent was obtained in accordance with the Declaration of Helsinki. Although the survey items in the present study were retrospectively examined, approval was obtained for research involving patients from the Institutional Review Board of Juntendo University Hospital (approval number: 13-058).
Data collection and measurements
We assessed age, sex, underlying diseases, coronary risk factors, left ventricular ejection fraction, body composition, muscle strength and exercise tolerance at the beginning of the CR, as described previously [15, 16]. Anthropometric parameters, including percentage of body fat, lean bodyweight and muscle mass were measured by bioelectrical impedance analysis (MC-780A; TANITA, Tokyo, Japan). In addition, we measured grip strength and a 6-min walking distance in the participants. Grip strength of both hands was measured in a standing position, and the higher grip strength value of the two hands was used. The 6-min walking test protocol was performed as previously described [3]. For blood biochemistry, parameters such as hemoglobin, albumin, creatinine, estimated glomerular filtration rate (eGFR), triglyceride, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), hemoglobin A1c (HbA1c), brain natriuretic peptide, and geriatric nutritional risk index (GNRI) were measured [17].
KCL
The KCL is a 25-item self-administrated questionnaire developed by the Japanese Ministry of Health, Labor and Welfare to identify frail older individuals who are at risk of requiring new certification for long-term care insurance [7]. The KCL comprises of seven types of questions aimed to assess the instrumental activities of daily living, physical function, nutritional status, oral function, social activities of daily living, cognitive function and depressive mood of participants. Thus, the KCL is a comprehensive evaluation method that focuses on the social and psychological aspects in addition to the physical aspects of frailty. Given its ability to assess frailty across multiple domains, the KCL is regarded as an effective screening tool [7]. The questions on the KCL require a simple “yes” or “no” answer, and are scored as 1 or 0 points, respectively. The patients were classified into three groups based on the KCL. Out of a maximum of 25 points, those with scores of ≥ 8 points were defined as the frailty group, those with 4 - 7 points are classified as the pre-frailty group, and those with ≤ 3 points as the non-frailty group [7].
Anxiety level
Anxiety levels were evaluated with a self-administered State Trait Anxiety Inventory Form (STAI) [18]. This form is an inventory consisting of 40 statements about the feelings of the participant, divided into two parts. In part I (consisting of 20 statements), patients are instructed to indicate the intensity of their feelings of anxiety at a particular moment (these indicate state anxiety), using scores ranging from 1 (absolutely not) to 4 (very much). In part II (other 20 statements), patients describe how they generally feel (these indicate trait anxiety) by reporting the frequency of their symptoms of anxiety, again using scores ranging from 1 (hardly ever) to 4 (often). The total score of each part may range between 20 and 80, with higher scores indicating higher levels of anxiety. In the present study, we used the Japanese version of the STAI [19].
Statistical analysis methods
Continuous variables are presented as mean ± standard deviation (SD). Differences among the three groups were analyzed by one-way analysis of variance (ANOVA) followed by Tukey’s honest significant difference test. The χ2 test was used to compare categorical variables. Spearman’s correlation coefficient was used to calculate the correlations between the KCL score and anxiety levels. Differences were considered significant when the P value was < 0.05. Statistical analysis was performed using the software JMP12.0 (SAS Institute Inc., Cary, NC, USA).
| Results | ▴Top |
Clinical characteristics of the patients
The clinical characteristics of the patients were presented in Table 1. Overall, the mean age of patients was 74.9 ± 5.8 years and 170 patients (67%) were males. There were 75 patients (29%) in the non-frailty group, 81 patients (32%) in the pre-frailty group, and 99 patients (39%) in the frailty group. Among the three groups, there were no significant differences in age, underlying disease or the prevalence of coronary risk factors. The frailty and pre-frailty groups consisted of a significantly lower proportion of male patients, and had lower lean body weight, 6-min walk distance and hemoglobin levels than those in the non-frailty group (P < 0.05 for all parameters). The frailty group also had significantly lower body mass index (BMI), GNRI and eGFR levels than those in the non-frailty group (P < 0.05 for all parameters).
 Click to view | Table 1. Clinical Characteristics of the Study Participants |
KCL score and anxiety level
Table 2 presented a comparison between the KCL scores and anxiety levels among the three groups. The pre-frailty group had significantly higher values in all sub-items except for instrumental activities of daily living when compared to the non-frailty group (P < 0.01 for all parameters). Furthermore, the frailty group had significantly higher values in all sub-items of the KCL when compared to the pre-frailty and the non-frailty groups (P < 0.01 for all parameters).
Click to view | Table 2. Comparison of Kihon Checklist Score and Anxiety Levels Among Three Groups |
State anxiety was significantly higher in the frailty groups when compared to the non-frailty group (41.6 ± 0.9 vs. 34.9 ± 1.0; P < 0.01). Trait anxiety increased in a stepwise manner across the three groups, and was significantly higher in the frailty and pre-frailty groups when compared to the non-frailty group (35.1 ± 1.1 vs. 39.2 ± 1.0 vs. 45.5 ± 0.9; P < 0.01).
The correlation between frailty scores and anxiety levels was presented in Figure 1. A significantly positive correlation was observed between the KCL score and state anxiety score (r = 0.32, P < 0.05; Fig. 1a) as well as between KCL score and trait anxiety score (r = 0.41, P < 0.05; Fig. 1b). A significantly positive correlation was also observed between the scores of items 1 to 20 of the KCL (excluding the depression items) and the state anxiety scores and trait anxiety scores (r = 0.23 vs. 0.33, P < 0.05; Fig. 1c, d).
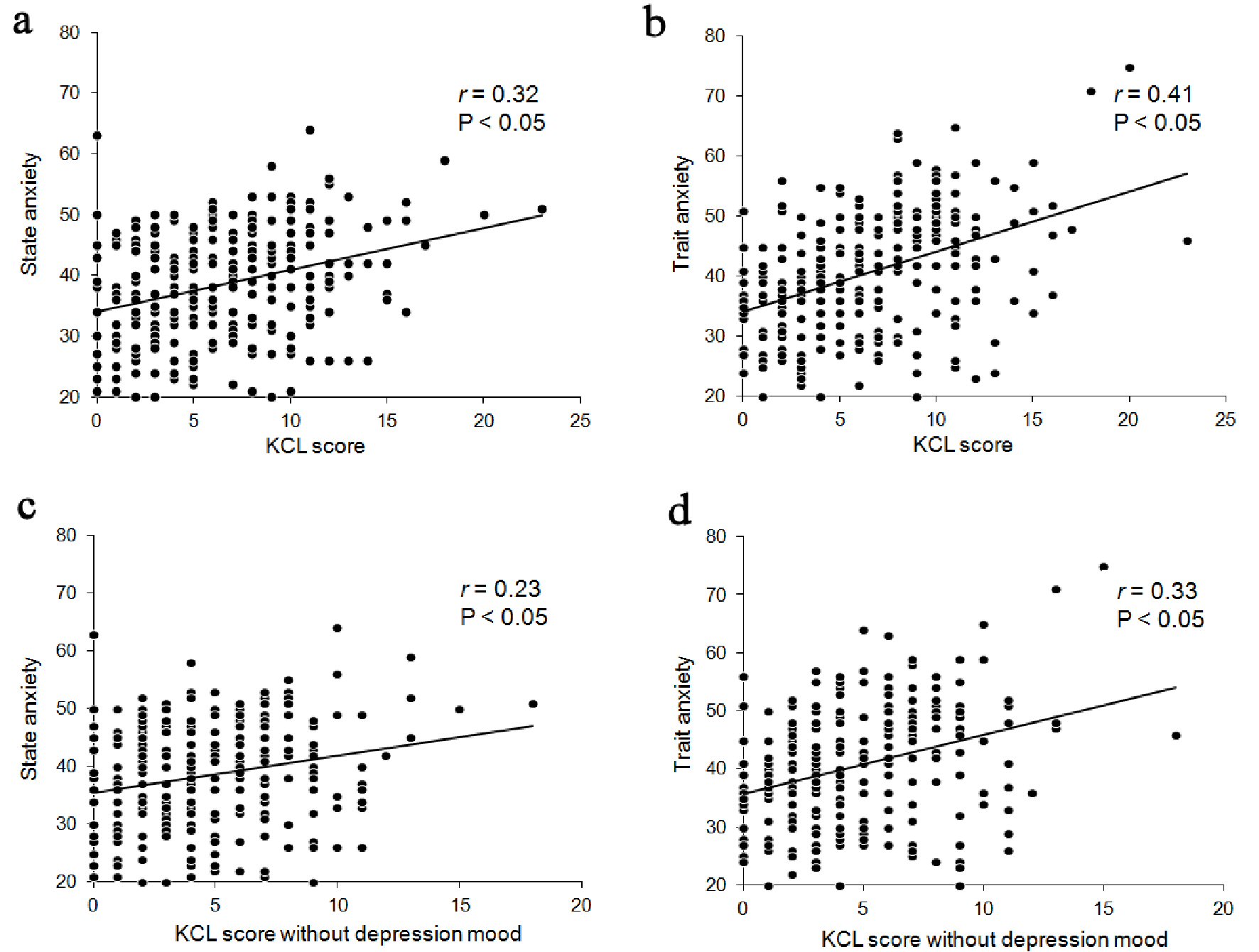 Click for large image | Figure 1. Correlation between KCL scores and anxiety levels. KCL score correlated with state anxiety (r = 0.32, P < 0.05) (a) and trait anxiety (r = 0.41, P < 0.05) (b) in elderly patients undergoing early phase II CR (n = 255). KCL score, excluding depression mood, correlated with state anxiety (r = 0.23, P < 0.05) (c) and trait anxiety (r = 0.33, P < 0.05) (d) in elderly patients undergoing early phase II CR (n = 255). KCL: Kihon Checklist. |
| Discussion | ▴Top |
In the present study, we demonstrated that the anxiety scores were significantly higher in the frailty and pre-frailty patients when compared to the non-frailty patients. We also demonstrated the relationship between the frailty score and anxiety levels in elderly patients undergoing early phase II CR. To the best of our knowledge, this is the first study demonstrating the relationship between frailty score and anxiety levels in elderly patients undergoing early phase II CR.
In Japan, the estimated rates of community-dwelling elderly individuals with frailty and pre-frailty are 6.9% and 49.6%, respectively [20]. Despite a high prevalence of pre-frailty in individuals with chronic disease and CVD, the rate of frailty in patients with CVD is estimated to be 25-50% [4, 21]. Indeed, the prevalence of frailty and pre-frailty were reported 39% and 32% in this study.
Frailty was related to the risk of mental health deterioration in community dwelling elderly individuals [22]. Pre-frailty was also found to be associated with emotional distress, including depression and anxiety [22]. Recent studies have also reported that anxiety and depression are predictors of pre-frailty to frailty progression [23, 24]. In addition, anxiety is an independent risk factor for exacerbation of disability in elderly individuals [25]. Moreover, elderly individuals who report depressive symptoms are at high risk of subsequent physical decline [26]. There is mutual risk relationship between physical frailty and psycho-emotional frailty such as cognitive dysfunction, dementia and depression [27, 28]. In the present study, KCL scores (excluding those from depression and mood; items 21 to 25) positively correlated with anxiety levels (Fig. 1c, d). These results support findings from previous reports [24].
Anxiety and depression co-exist at a high rate in patients with heart failure [10]. Additionally, the presence of anxiety also promotes depression [29]. Furthermore, Andreescu et al have demonstrated that a decline in cognitive function also correlates with anxiety in elderly patients [30]. Anxiety, depression, and cognitive function are all multi-dimensional entities, interacting in complex ways within the neural mechanisms [30]. Another previous report has proposed that apathy and anxiety should be considered in clinical practice as psychological symptoms observed in frailty elderly individuals, in addition to depression and dementia [31]. Therefore, we believe that it is important to perform complex evaluations integrating psycho-emotional and cognitive function, particularly in elderly individuals.
The mechanism by which anxiety can be a risk factor for CVD is controversial. Depression and anxiety have increased physiological impairments, such as dysfunction of the autonomic nervous system and platelet activation disorders of the hypothalamic-pituitary-adrenal axis [32]. Furthermore, higher anxiety is associated with behavioral issues such as inactivity, reduced ability for selfcare, smoking and poor adherence to CR [32, 33]. We believe that evaluating the levels of anxiety is also important in order to understand the behavior of elderly patients who are undergoing CR and to determine ways to help them cope with the condition.
The present study had several limitations. First, this was a single-center study with a small sample size, which limits the possibility of generalizing the results. Second, psycho-emotional states, including anxiety and depression, might be difficult to completely distinguish because they were associated with cognitive function and are also interrelated. Third, this study was a cross-sectional design. Therefore, we were unable to prove any causal relationships between frailty score and anxiety level. Thus, these findings require further examination, possibly involving several screening tools.
Conclusions
Frailty was positively correlated with depression and anxiety levels in elderly patients undergoing early phase II CR. The assessment of depressive mood and anxiety was also recognized to be important in elderly patients undergoing early phase II CR.
Acknowledgments
The authors thank all study participants and members who carried out data collection in Cardiovascular Rehabilitation and Fitness. This study was supported in part by JSPS KAKENHI (grant number 17K01470 and 19K11374), and the High Technology Research Center Grant from the Ministry of Education, Culture, Science and Technology, Japan.
Financial Disclosure
The authors declare that the present article has not benefitted from any source of funding.
Conflict of Interest
The authors do not have any conflict of interest to declare concerning the present article.
Informed Consent
All patients provided written informed consent.
Author Contributions
AH has designed and performed the study. AH, MN-Y, and KS have drafted the manuscript and did critical editing. AH, MN-Y, MK, MY, TM, RM, AA, TA, SO, MS, YS, KF, AS, TY, AA, TA, MS, TM, TT, TF, HD, and TM have assisted and supported in sample collection. MN-Y and KS have carefully supervised this manuscript preparation and writing.
Data Availability
The data sets will not be publicly available because patient consent in our institute does not allow for such publication. The corresponding author will respond to inquiries on data analyses.
| References | ▴Top |
- Shimokawa H, Miura M, Nochioka K, Sakata Y. Heart failure as a general pandemic in Asia. Eur J Heart Fail. 2015;17(9):884-892.
doi pubmed - Cacciatore F, Abete P, Mazzella F, Viati L, Della Morte D, D'Ambrosio D, Gargiulo G, et al. Frailty predicts long-term mortality in elderly subjects with chronic heart failure. Eur J Clin Invest. 2005;35(12):723-730.
doi pubmed - Boxer R, Kleppinger A, Ahmad A, Annis K, Hager D, Kenny A. The 6-minute walk is associated with frailty and predicts mortality in older adults with heart failure. Congest Heart Fail. 2010;16(5):208-213.
doi pubmed - Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, Seeman T, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56(3):M146-156.
doi pubmed - Vellas B, Balardy L, Gillette-Guyonnet S, Abellan Van Kan G, Ghisolfi-Marque A, Subra J, Bismuth S, et al. Looking for frailty in community-dwelling older persons: the Gerontopole Frailty Screening Tool (GFST). J Nutr Health Aging. 2013;17(7):629-631.
doi pubmed - Sewo Sampaio PY, Sampaio RA, Yamada M, Arai H. Systematic review of the Kihon checklist: is it a reliable assessment of frailty? Geriatr Gerontol Int. 2016;16(8):893-902.
doi pubmed - Satake S, Senda K, Hong YJ, Miura H, Endo H, Sakurai T, Kondo I, et al. Validity of the Kihon Checklist for assessing frailty status. Geriatr Gerontol Int. 2016;16(6):709-715.
doi pubmed - Shimada K. Editorial: Sudden cardiovascular events and comprehensive cardiac rehabilitation: come back from "a bolt out of the blue". J Cardiol Cases. 2015;11(6):164-165.
doi pubmed - Hanssen TA, Nordrehaug JE, Eide GE, Bjelland I, Rokne B. Anxiety and depression after acute myocardial infarction: an 18-month follow-up study with repeated measures and comparison with a reference population. Eur J Cardiovasc Prev Rehabil. 2009;16(6):651-659.
doi pubmed - Yohannes AM, Willgoss TG, Baldwin RC, Connolly MJ. Depression and anxiety in chronic heart failure and chronic obstructive pulmonary disease: prevalence, relevance, clinical implications and management principles. Int J Geriatr Psychiatry. 2010;25(12):1209-1221.
doi pubmed - Kubzansky LD, Cole SR, Kawachi I, Vokonas P, Sparrow D. Shared and unique contributions of anger, anxiety, and depression to coronary heart disease: a prospective study in the normative aging study. Ann Behav Med. 2006;31(1):21-29.
doi pubmed - Barefoot JC, Helms MJ, Mark DB, Blumenthal JA, Califf RM, Haney TL, O'Connor CM, et al. Depression and long-term mortality risk in patients with coronary artery disease. Am J Cardiol. 1996;78(6):613-617.
doi - Guidelines for cardiac rehabilitation in patients with cardiovascular disease (JCS2012). Available online: http://www.j-circ.or.jp/guideline/pdf/JCS2012_nohara_h.pdf (Accessed on March 25, 2000).
- Nishitani M, Shimada K, Masaki M, Sunayama S, Kume A, Fukao K, Sai E, et al. Effect of cardiac rehabilitation on muscle mass, muscle strength, and exercise tolerance in diabetic patients after coronary artery bypass grafting. J Cardiol. 2013;61(3):216-221.
doi pubmed - Nishitani-Yokoyama M, Miyauchi K, Shimada K, Miyazaki T, Ogita M, Okazaki S, Shioya M, et al. Effects of phase II comprehensive cardiac rehabilitation on coronary plaque volume after acute coronary syndrome. Int Heart J. 2015;56(6):597-604.
doi pubmed - Nishitani-Yokoyama M, Miyauchi K, Shimada K, Yokoyama T, Ouchi S, Aikawa T, Kunimoto M, et al. Impact of physical activity on coronary plaque volume and components in acute coronary syndrome patients after early phase ii cardiac rehabilitation. Circ J. 2018;83(1):101-109.
doi pubmed - Sugita Y, Miyazaki T, Shimada K, Shimizu M, Kunimoto M, Ouchi S, Aikawa T, et al. Correlation of nutritional indices on admission to the coronary intensive care unit with the development of delirium. Nutrients. 2018;10(11):1712.
doi pubmed - Spielberger CD, Gorsuch RL, Lushene RE. Manual of the state trait anxiety inventory. Consulting Psychologists Press. 1983:19-55.
doi - Hidano T, Fukuhara M, Iwawaki S, Soga S, Spielberger CD. State-trait anxiety inventory-form JYZ. Tokyo, Japan: Jitsumu Kyoiku Shuppan. 2000.
- Makizako H, Shimada H, Doi T, Tsutsumimoto K, Suzuki T. Impact of physical frailty on disability in community-dwelling older adults: a prospective cohort study. BMJ Open. 2015;5(9):e008462.
doi pubmed - Afilalo J. Frailty in patients with cardiovascular disease: why, when, and how to measure. Curr Cardiovasc Risk Rep. 2011;5(5):467-472.
doi pubmed - Ni Mhaolain AM, Fan CW, Romero-Ortuno R, Cogan L, Cunningham C, Kenny RA, Lawlor B. Frailty, depression, and anxiety in later life. Int Psychogeriatr. 2012;24(8):1265-1274.
doi pubmed - Gordon SJ, Baker N, Kidd M, Maeder A, Grimmer KA. Pre-frailty factors in community-dwelling 40-75 year olds: opportunities for successful ageing. BMC Geriatr. 2020;20(1):96.
doi pubmed - Bernal-Lopez C, Potvin O, Avila-Funes JA. Frailty is associated with anxiety in community-dwelling elderly adults. J Am Geriatr Soc. 2012;60(12):2373-2374.
doi pubmed - Brenes GA, Guralnik JM, Williamson JD, Fried LP, Simpson C, Simonsick EM, Penninx BW. The influence of anxiety on the progression of disability. J Am Geriatr Soc. 2005;53(1):34-39.
doi pubmed - Penninx BW, Guralnik JM, Ferrucci L, Simonsick EM, Deeg DJ, Wallace RB. Depressive symptoms and physical decline in community-dwelling older persons. JAMA. 1998;279(21):1720-1726.
doi pubmed - Kulmala J, Nykanen I, Manty M, Hartikainen S. Association between frailty and dementia: a population-based study. Gerontology. 2014;60(1):16-21.
doi pubmed - Makizako H, Shimada H, Doi T, Yoshida D, Anan Y, Tsutsumimoto K, Uemura K, et al. Physical frailty predicts incident depressive symptoms in elderly people: prospective findings from the Obu study of health promotion for the elderly. J Am Med Dir Assoc. 2015;16(3):194-199.
doi pubmed - Suzuki T, Shiga T, Kuwahara K, Kobayashi S, Suzuki S, Nishimura K, Suzuki A, et al. Impact of clustered depression and anxiety on mortality and rehospitalization in patients with heart failure. J Cardiol. 2014;64(6):456-462.
doi pubmed - Andreescu C, Teverovsky E, Fu B, Hughes TF, Chang CC, Ganguli M. Old worries and new anxieties: behavioral symptoms and mild cognitive impairment in a population study. Am J Geriatr Psychiatry. 2014;22(3):274-284.
doi pubmed - Ma L. Depression, anxiety, and apathy in mild cognitive impairment: current perspectives. Front Aging Neurosci. 2020;12:9.
doi pubmed - Moser DK, Arslanian-Engoren C, Biddle MJ, Chung ML, Dekker RL, Hammash MH, Mudd-Martin G, et al. Psychological aspects of heart failure. Curr Cardiol Rep. 2016;18(12):119.
doi pubmed - Harris KM, Anderson DR, Landers JD, Emery CF. Higher anxiety and will to live are associated with poorer adherence to cardiac rehabilitation. J Cardiopulm Rehabil Prev. 2019;39(6):381-385.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.