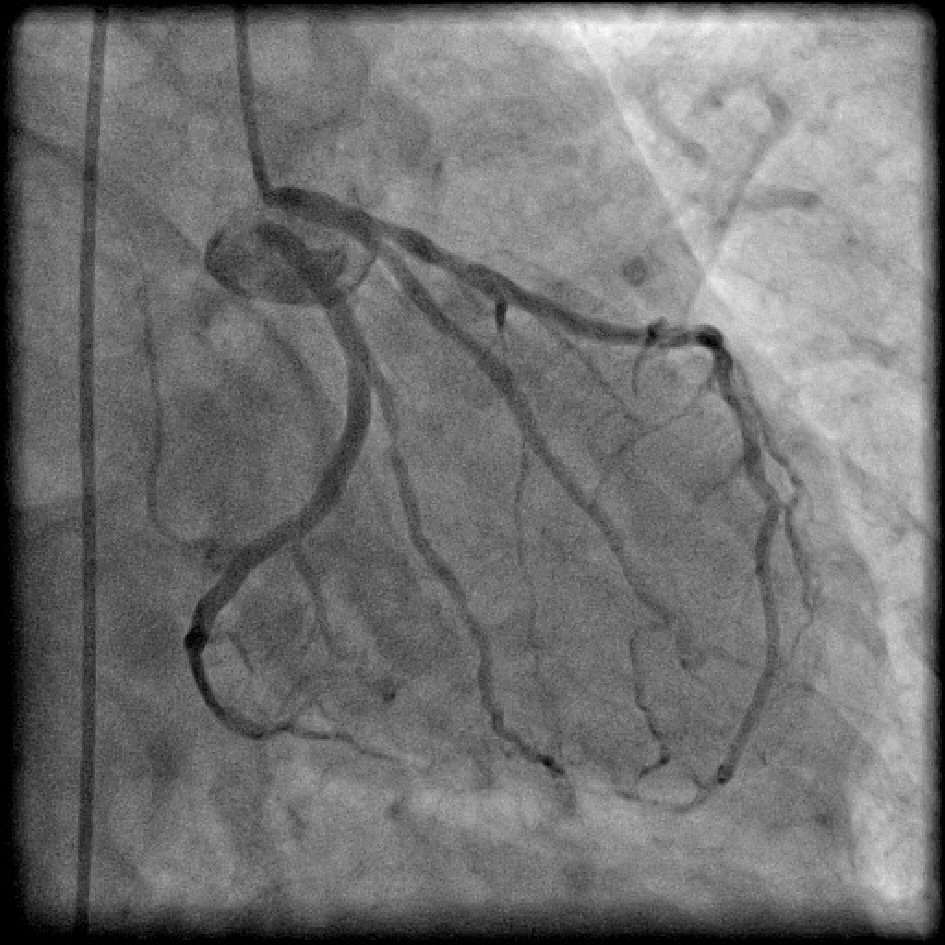
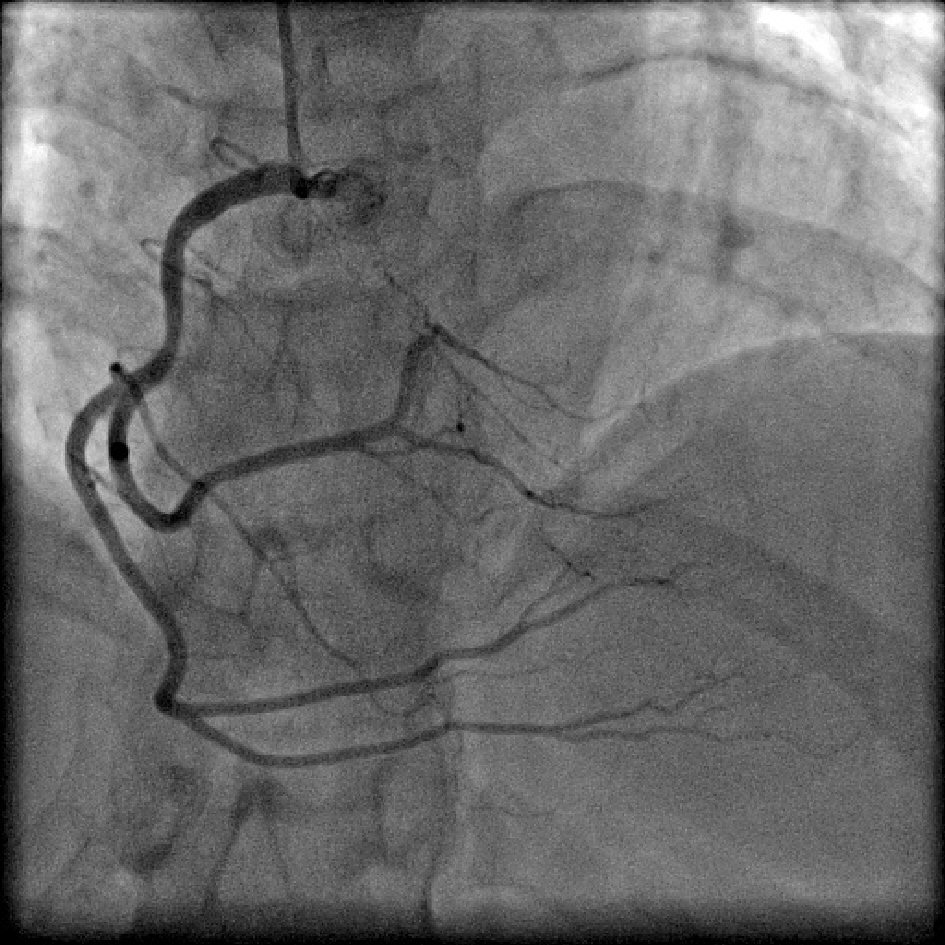
Figure 1. Coronary angiogram in right anterior oblique (RAO) caudal projection showing absent left main trunk with separate origin of left anterior descending artery (LAD) and left circumflex (LCX) from left sinus.
| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website http://www.cardiologyres.org |
Original Article
Volume 10, Number 6, December 2019, pages 358-368
Incidence, Characteristics and Atherosclerotic Involvement of Coronary Artery Anomalies in Adult Population Undergoing Catheter Coronary Angiography
Figures
Tables
| LAD: left anterior descending artery; RCA: right coronary artery; LCA: left coronary artery. |
| Anomalies of origin and course |
| Absent left main trunk |
| Anomalous location of coronary ostium within aortic root or adjacent to proper aortic sinus |
| Anomalous location of coronary ostium outside normal coronary sinuses |
| Anomalous location of coronary ostium at improper sinus |
| Single coronary artery |
| Anomalies of intrinsic coronary arterial anatomy |
| Congenital ostial stenosis or atresia |
| Coronary ostial dimple |
| Coronary ectasia or aneurysm |
| Absent coronary artery |
| Coronary hypoplasia |
| Intramural coronary artery (myocardial bridging) |
| Subendocardial coronary course |
| Coronary crossing |
| Anomalous origin of posterior descending artery from LAD or from a septal branch |
| Split RCA |
| Split LAD/dual LAD |
| Ectopic origination of first septal branch |
| Anomalies of coronary termination |
| Inadequate arteriolar/capillary ramifications |
| Fistulas from RCA, LCA, or conus artery |
| Anomalous anastomotic vessels |
| Clinical characteristics | N (%) |
|---|---|
| LV: left ventricle. | |
| Gender | |
| Male | 74 (74.75%) |
| Female | 25 (25.25%) |
| Indication for coronary angiography | |
| Acute coronary syndromes | 43 (43.43%) |
| Stable ischemic heart disease (angina/dyspnea on exertion) | 25 (25.25%) |
| Atypical chest pain with Electrocardiographic/ Echocardiographic changes | 22 (22.22%) |
| Heart failure or LV dysfunction | 7 (7.07%) |
| Workup prior to pacemaker implantation | 2 (2.02%) |
| Risk factors | |
| Hypertension | 41 (41.41%) |
| Diabetes mellitus | 33 (33.33%) |
| Dyslipidemia | 19 (19.19%) |
| Smoking | 26 (26.26%) |
| Anomaly | N | Incidence (%) | Anomaly (%) |
|---|---|---|---|
| aUsually benign. bPotentially serious. cSmall fistulae are usually benign, large or multiple fistulae can lead to serious manifestations. LAD: left anterior descending artery; RCA: right coronary artery; LCX: left circumflex artery; PDA: posterior descending artery. | |||
| Total coronary angiographies | 3,233 | ||
| Total coronary anomalies | 99 | 3.06 | |
| Anomalies of origin and distribution | |||
| Absent left main trunka | 14 | 0.43 | 14.14 |
| RCA from left sinusb | 12 | 0.37 | 12.12 |
| RCA from ascending aortaa | 4 | 0.12 | 4.04 |
| LCX from right sinus/RCAa | 13 | 0.40 | 13.13 |
| Anomalies of intrinsic coronary arterial anatomy | |||
| Split RCAa | 27 | 0.84 | 27.27 |
| Dual LADa | 22 | 0.68 | 22.22 |
| Superdominant LAD supplying PDAa | 1 | 0.03 | 1.01 |
| Anomalies of coronary termination | |||
| Coronary arterial fistulaec | 6 | 0.18 | 6.06 |
| Total number | Percentage (%) | |
|---|---|---|
| CAAs: coronary artery anomalies; CAD: coronary artery disease; LMCA: left main coronary artery. | ||
| Total patients with CAAs | 99 | 100 |
| Normal coronaries/insignificant CAD | 31 | 31.31 |
| Significant CAD | 68 | 68.69 |
| Single vessel disease | 20 | 20.20 |
| Double vessel disease | 18 | 18.18 |
| Triple vessel disease | 30 | 30.30 |
| LMCA involvement | 1 | 1.01 |
| Patients with CAD in anomalous vessels | 53 | 53.54 |
| Patients with CAD only in normal vessels | 15 | 15.15 |
| Patients with CAD only in anomalous vessels | 11 | 11.11 |
| Author/year of publication | Incidence (%) | Most common anomaly | Imaging modality | Country |
|---|---|---|---|---|
| LM: left main; LAD: left anterior descending artery; LCX: left circumflex artery; RCA: right coronary artery; RCS: right coronary sinus; LCS: left coronary sinus; NCS: non-coronary sinus; CAG: catheter coronary angiography; MDCT: multidetector computed tomography. | ||||
| Yamanaka et al, 1990 [2] | 1.30 (1,686 of 126,595) | Absent LM trunk with separate origin of LAD and LCX | CAG | USA |
| Kaku et al, 1996 [8] | 0.31 (56 of 17,731) | Anomalous origin of RCA from LCS | CAG | Japan |
| Kardos et al, 1997 [7] | 1.34 (103 of 7,694) | Absent LM trunk with separate origin of LAD and LCX | CAG | Central Europe |
| Garg et al, 2000 [9] | 0.95 (39 of 4,100) | Anomalous origin of RCA from LCS/NCS | CAG | India |
| Angelini et al, 2002 [10] | 5.64 (110 of 1,950) | Split RCA | CAG | USA |
| Yildiz et al, 2010 [3] | 0.90 (112 of 12,457) | Absent LM trunk with separate origin of LAD and LCX | CAG | Turkey |
| Erol et al, 2011 [11] | 1.96 (53 of 2,096) | Absent LM trunk with separate origin of LAD and LCX/origin of RCA from LCS | MDCT | Turkey |
| Fujimoto et al, 2011 [12] | 1.52 (89 of 5,869) | Anomalous origin of RCA from LCS | MDCT | Japan |
| Sivri et al, 2012 [35] | 0.74 (95 of 12,814) | Anomalous origin of LCX from RCS/RCA | CAG | Turkey |
| Sohrabi et al, 2012 [27] | 1.30 (79 of 6,065) | Absent LM trunk with separate origin of LAD and LCX | CAG | Iran |
| Xu et al, 2012 [36] | 1.02 (124 of 12,415) | Anomalous origin of RCA from LCS | CTCA | China |
| Yuksel et al, 2013 [13] | 0.29 (48 of 16,573) | Anomalous origin of LCX from RCS/RCA | CAG | Turkey |
| Namgung et al, 2014 [37] | 1.16 (103 of 8,864) | Anomalous origin of RCA from LCS | MDCT | Korea |
| Tharwat et al, 2014 [23] | 2.7 (115 of 4,246) | Anomalous origin of LCX from RCS/RCA | CAG | Egypt |
| Altin et al, 2015 [38] | 1.4 (78 of 5,548) | Absent LM trunk with separate origin of LAD and LCX | CAG | Turkey |
| Sivakumar et al, 2017 [28] | 2.06 (32 of 1,547) | Anomalous origin of RCA from LCS | CAG | India |
| Somashekhara, 2017 [24] | 0.65 (162 of 25,023) | Anomalous origin of RCA from LCS | CAG | India |
| Nawale et al, 2018 [29] | 1.91 (86 of 4,481) | Anomalous origin of RCA from LCS/NCS | CAG | India |