Figures
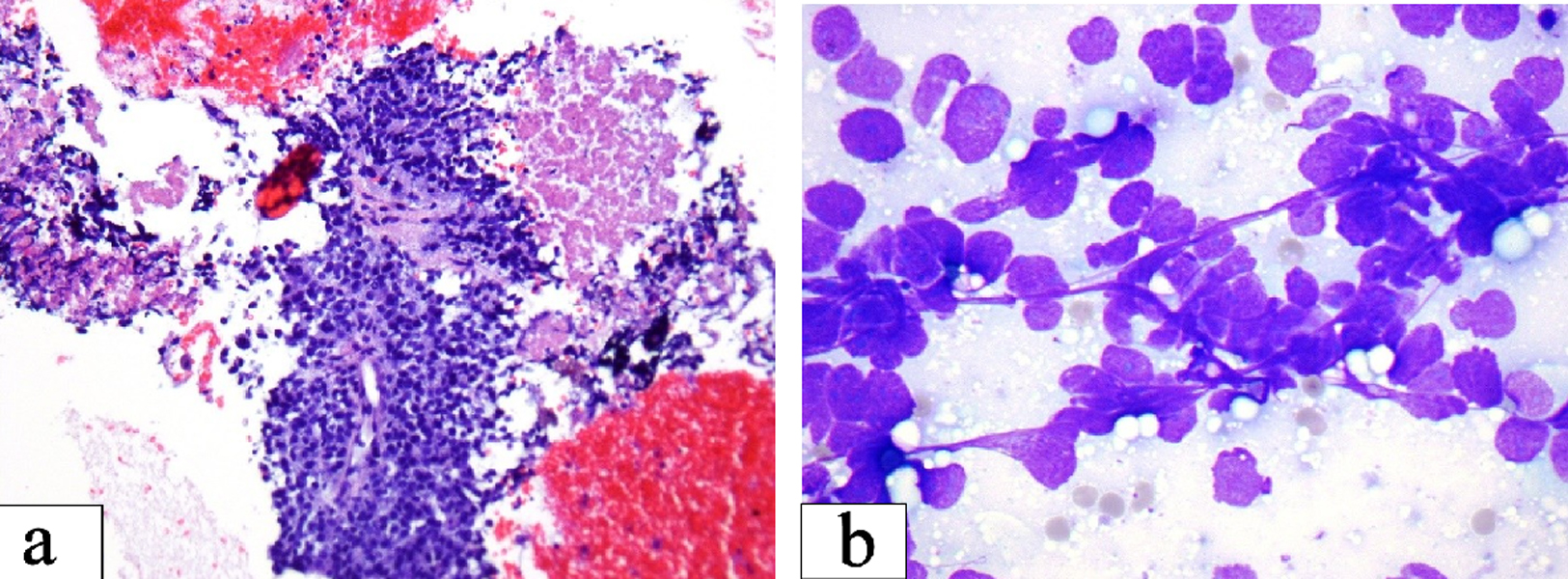
Figure 1. (a) Small cell carcinoma: loosely cohesive clusters of small cells with high nuclear cytoplasmic ratio and fine chromatin. Streaks of nuclear material and nuclear molding as seen are important diagnostic clue (Smear, Diff-Quik stain, × 600). (b) Necrosis seen as granular pink material in the upper right corner may be prominent. The center of the field shows preserved tumor cells with high nuclear cytoplasmic ratio around capillaries (Cell block section, H&E stain, × 200).

Figure 2. CT imaging of the brain demonstrating new mild hypodensities in the right subcortical frontal lobe, stable milder hypodensities in the left subcortical frontal lobe, stable hypodensities in the left occipital lobe, and minimal periventricular white matter hypodensities.
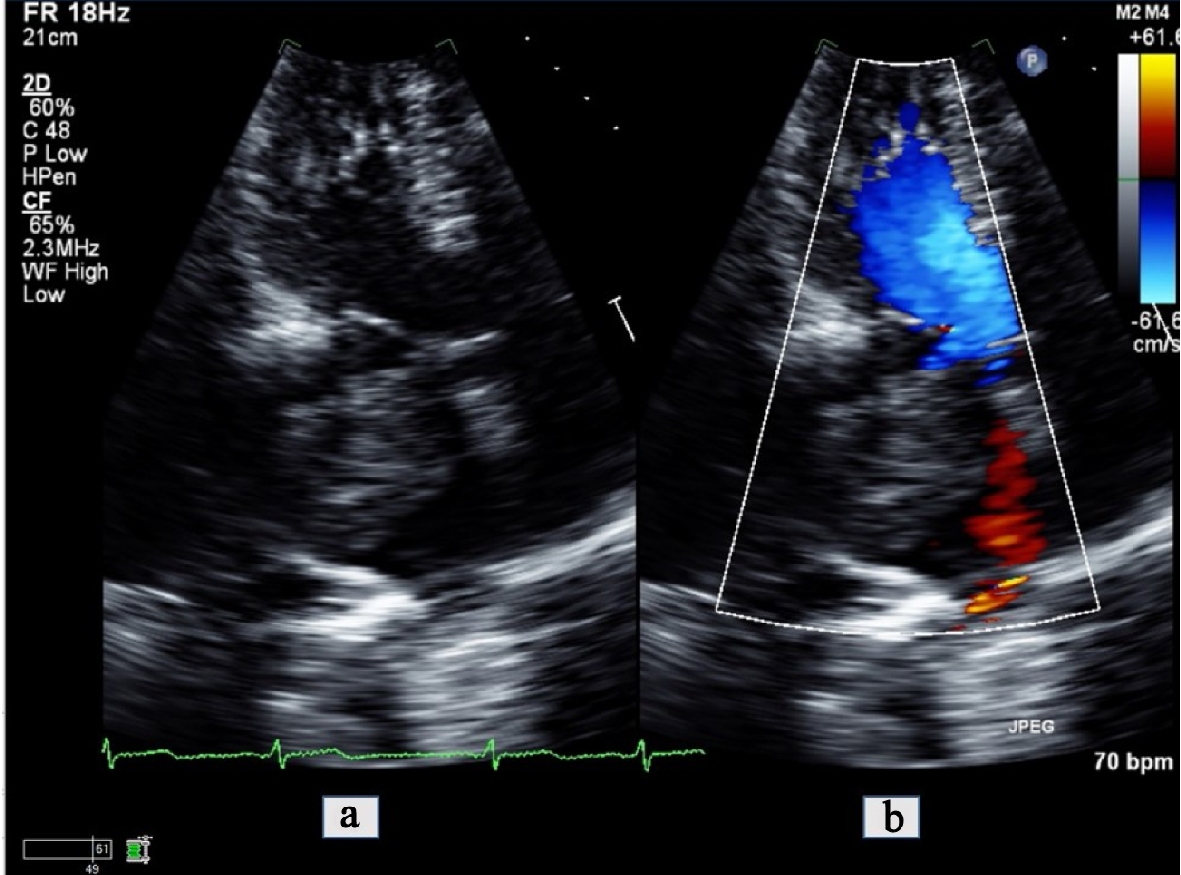
Figure 3. Apical 4-chamber view transthoracic echocardiogram zoomed in on the left atrium (a) with color comparison (b) showing a large tumor invading into the left atrial cavity.
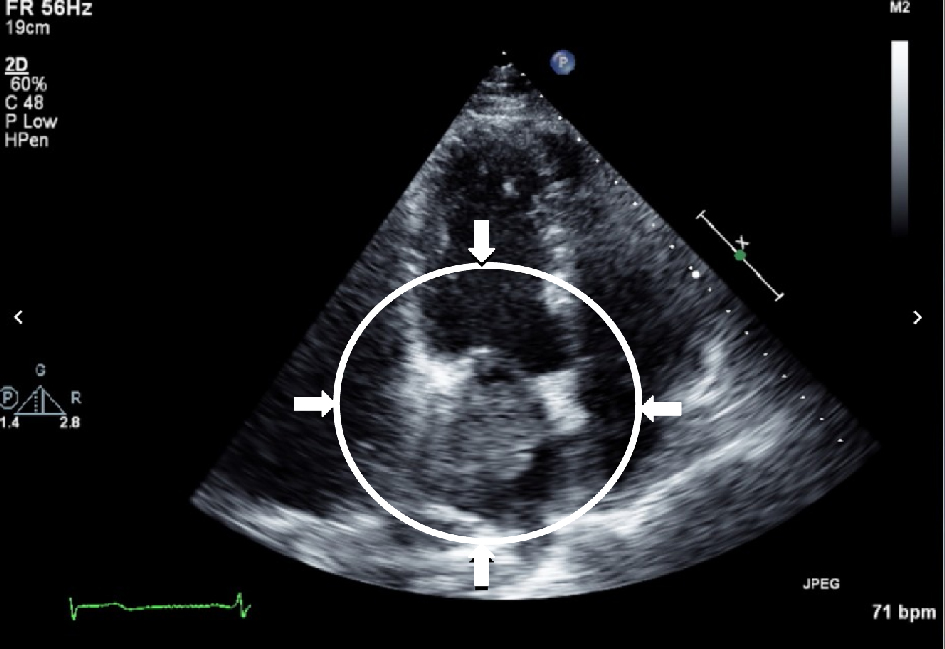
Figure 4. Transthoracic echocardiogram demonstrating infiltrating mass in the left atrium with possible extension through the mitral valve into the left ventricle.
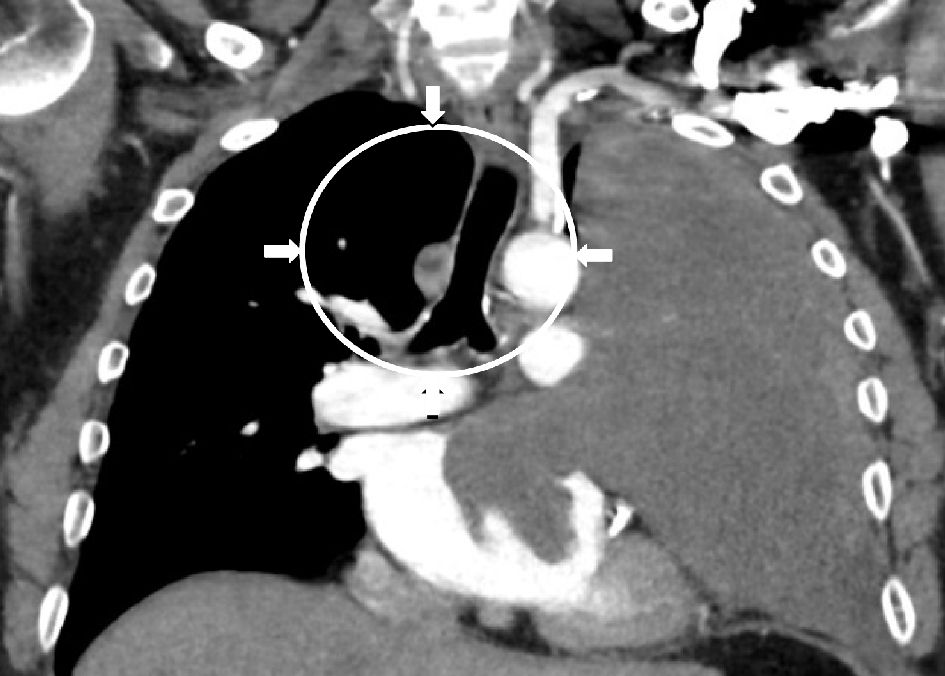
Figure 5. CT imaging with contrast of the chest demonstrating the large soft tissue map entirely displacing the left upper lobe of the lung with encasement of the left main pulmonary artery and invasion of both the left upper anterior pulmonary vein and left atrial cavity. The lesion abuts the left aortic arch, main pulmonary trunk, and the left cardiac border.

Figure 6. Upright frontal and lateral X-rays demonstrating large, left-sided hilar mass.