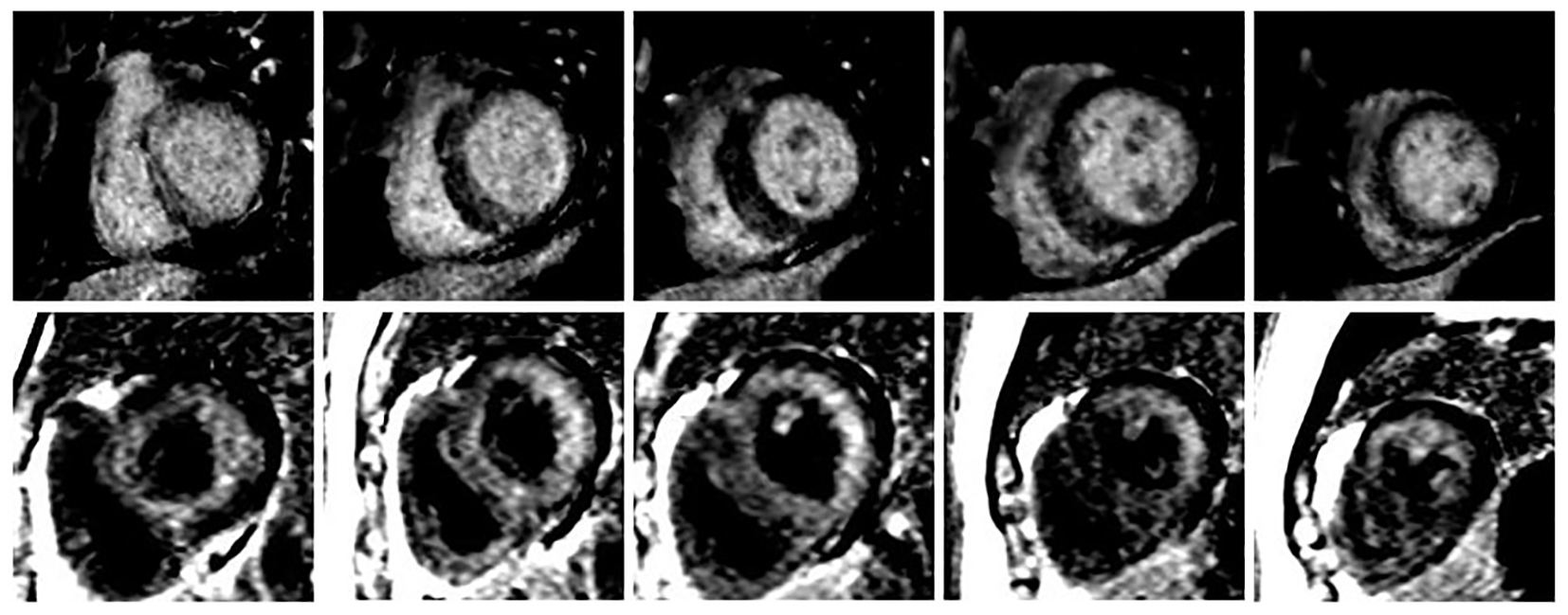
Figure 1. Different LGE patterns between two CMRs. The upper panel showed mid-myocardial delayed enhancement in first CMR (October 2015), and the lower panel showed global subendocardial enhancement in second CMR (March 2016).
| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Case Report
Volume 7, Number 5, October 2016, pages 178-180
Cardiac Amyloidosis Masked as Hypertrophic Cardiomyopathy: A Case Report
Figure
Table
| 2015 | 2016 | |
|---|---|---|
| IVS: interventricular septum; LVEF: left ventricular ejection fraction; CMR: cardiac magnetic resonance; LGE: late gadolinium enhancement. | ||
| ECG | Sinus rhythm Normal QRS voltage Q waves in the inferior leads and from V1 to V4 | Sinus rhythm Low QRS voltages Q waves in the inferior leads and from V1 to V4 |
| Echocardiography | IVS thickness: 1.6 cm Normal LVEF of 61% Dilated LA Severe diastolic dysfunction | IVS thickness: 1.6 cm Normal LVEF of 55% Dilated LA Severe diastolic dysfunction |
| CMR | Moderate hypertrophy without obstruction (IVS thickness 1.6 cm) Normal size with mildly decreased cardiac function (LVEF 46%) Pattern of LGE: faint mid-myocardial delayed enhancement at the infero-septum from base to mid-cavity | Mildly hypertrophy without obstruction (IVS thickness 1.2 cm) Normal size with global hypokinesis (LVEF 41%) Pattern of LGE: subendocardial enhancement |
| Diagnosis | Hypertrophic cardiomyopathy | Cardiac amyloidosis |