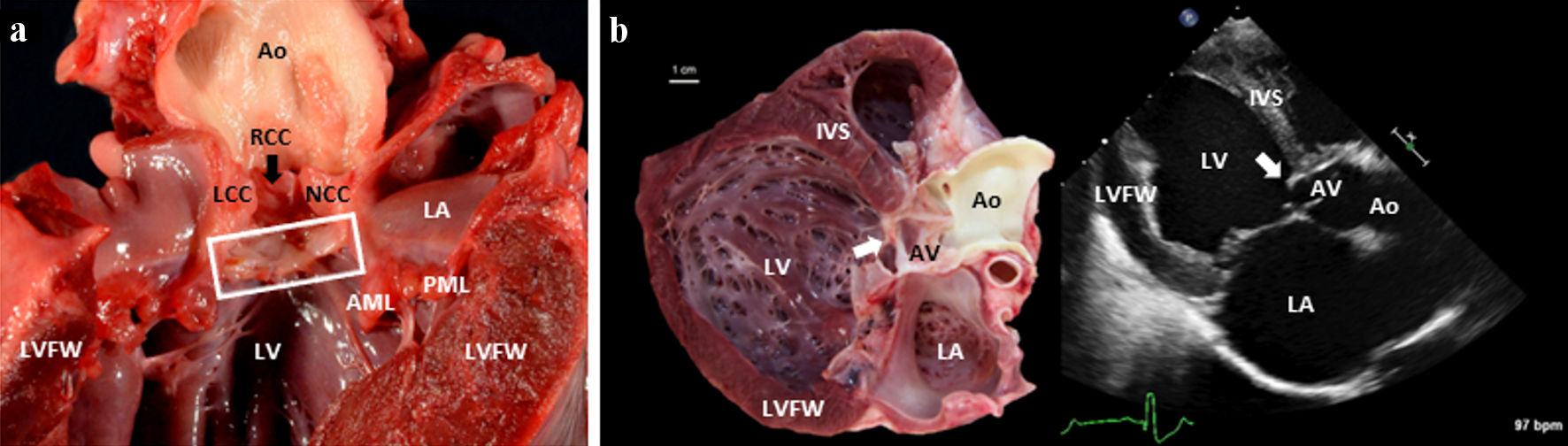
Figure 1. (a) A gross pathology image of the left side of a canine heart affected with SAS. The heart was incised along the long axis of the heart, from the apex to the base (transecting the LVFW). A box surrounds the subvalvular aortic ridge. A black arrow indicates the RCC. (b) A paired gross image and a 2D echocardiographic image (from a right parasternal long-axis five-chamber view) of an 8-month-old Mastiff dog heart afflicted by severe SAS. In both images, you can see the white (gross pathology specimen) and bright (2D echocardiographic image) severe subvalvular ridge/ring of tissue indicated by the white arrow. Note that the specimen shows a dilated and concentrically hypertrophied left ventricle in response to the pressure overload of SAS and the volume overload of concomitant severe AI and mitral valve regurgitation. 2D: two-dimensional; AML: anterior mitral leaflet; Ao: aorta; IVS: interventricular septum; LA: left atrium; LCC: left coronary cusp; LV: left ventricular lumen; LVFW: left ventricular free wall; LVOT: left ventricular outflow tract; NCC: noncoronary cusp; PML: posterior mitral leaflet; RCC: right coronary cusp; SAS: subvalvular aortic stenosis.