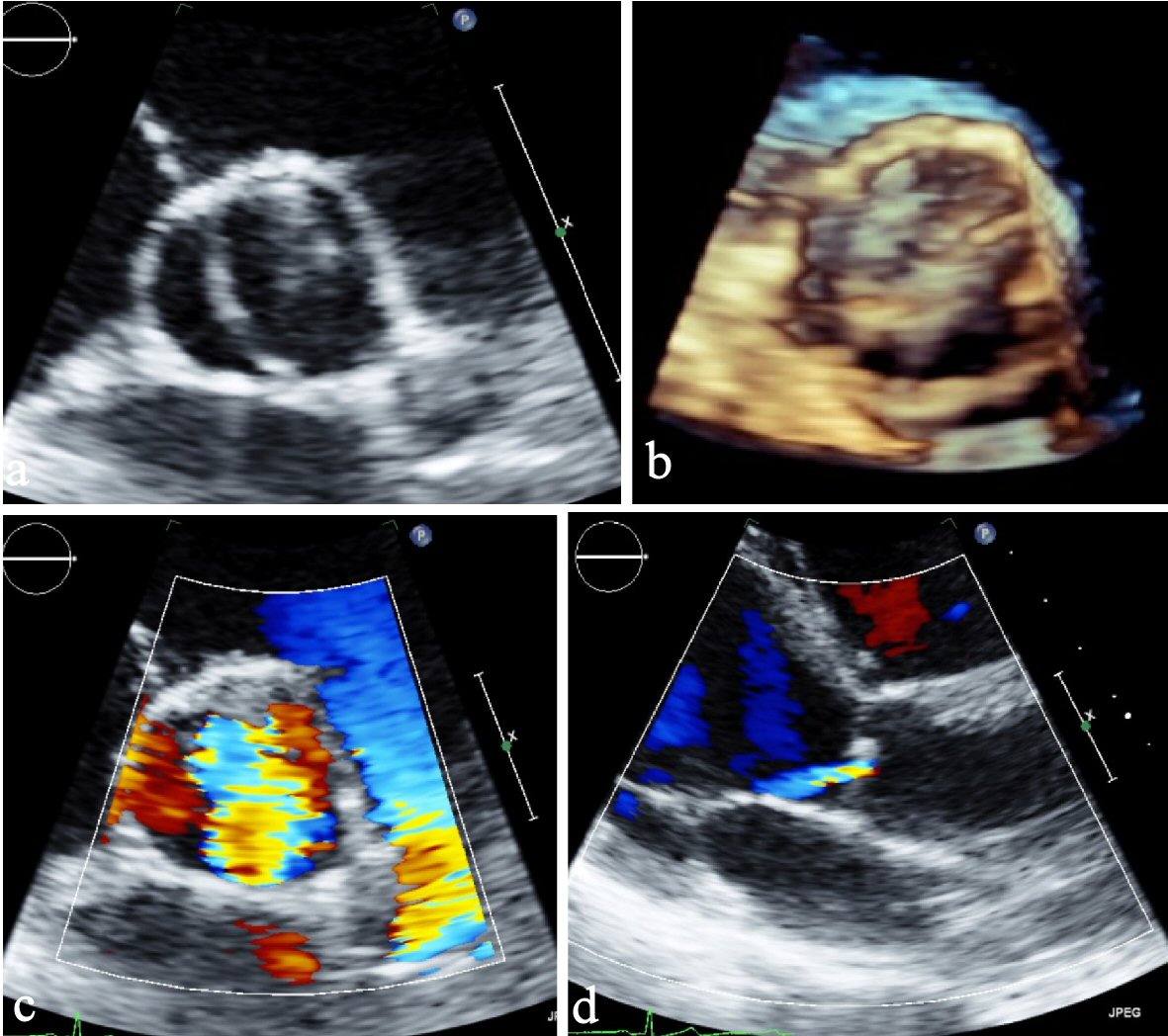
Figure 1. (a) Parasternal short axis view. (b) Parasternal short axis view (3D). (c) Parasternal short axis view of color Doppler showing severe aortic insufficiency. (d) Parasternal long axis view showing eccentric jet of regurgitant flow typical by BAV. BAV: bicuspid aortic valve; 3D: three-dimensional.