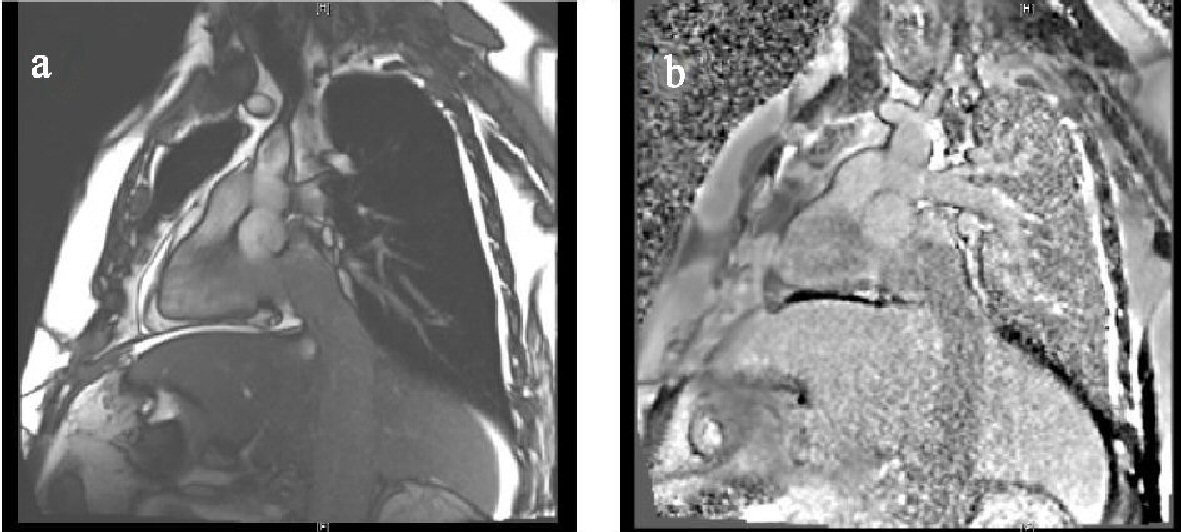
Figure 1. MRI pre and post contrast. (a) and (b): A large oval mass measuring 5 × 4.2 cm is visualized within the right atrium. The borders appear to be fairly regular. This mass appears to be in continuity with its extension into the inferior vena cava. A small to medium-sized circumferential pericardial effusion is present without changes of tamponade. The left ventricle is small in size with mild left ventricular hypertrophy. The inferior vena cava is dilated and filled up by echogenic material, likely malignancy.
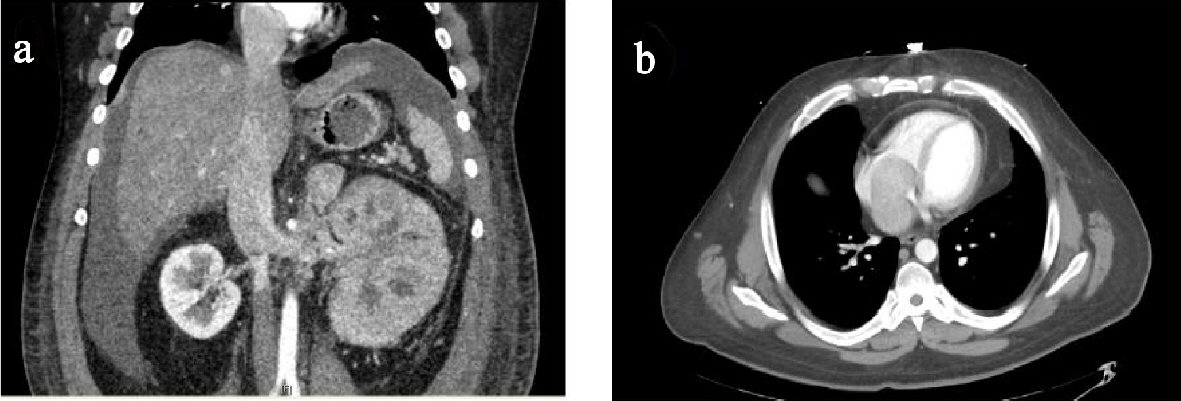
Figure 2. CT chest and abdomen with contrast. (a) and (b): Extensive heterogeneous masslike enlargement of the left kidney, associated with altered areas of cortical thickening/enhancement and architectural distortion. Masslike expansion of the left renal vein and inferior vena cava, extending into the right atrium is suggestive of extensive propagation of enhancing tumor thrombus. Masslike enlargement of the left adrenal gland measuring 3.3 × 3.2 cm and multiple small hypervascular nodules throughout the liver, most compatible with metastatic disease.
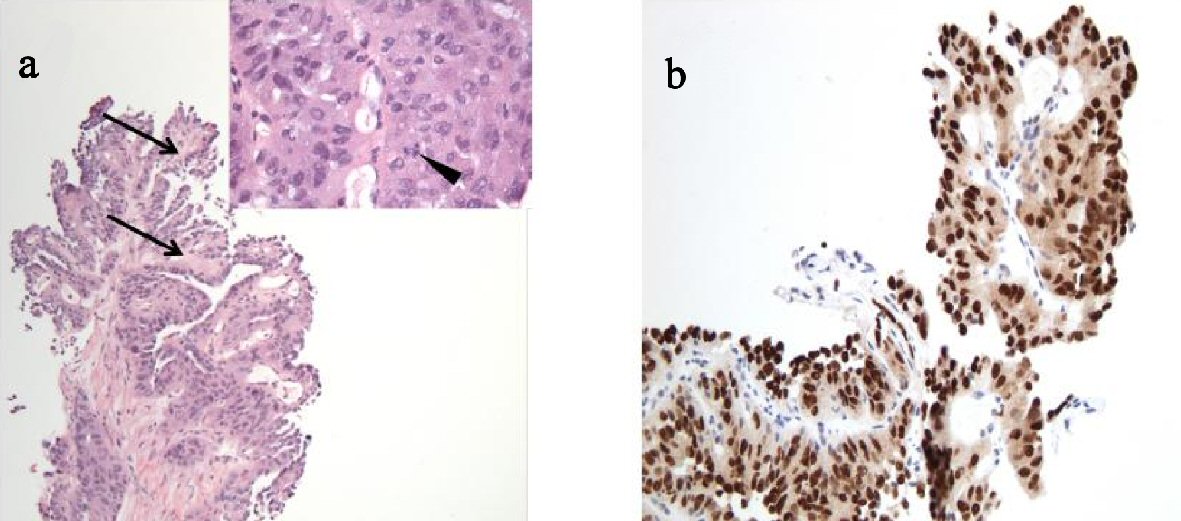
Figure 3. Adrenal biopsy. (a) H&E stain (100 × total magnification) and inset (400 × total magnification). The tumor demonstrates papillary architecture, as evidenced by tumor cells lining fibrovascular cores (arrows). The inset shows tumor cells with abundant eosinophilic cytoplasm, nuclear pleomorphism and mitotic activity (arrowhead) and lacking glandular formation. Importantly, morphologic features of clear cell renal cell carcinoma are not identified. (b) Adrenal biopsy, Pax-8 immunohistochemical stain (200 × total magnification). Pax-8 is a nuclear transcription factor, which labels tissue of renal, thymic and thyroid origin and is therefore useful for identifying metastatic tumors from these sites. In the clinical context of a patient with a large renal mass, the strong nuclear positivity (brown staining of the tumor cell nuclei) is supportive of origin of this metastatic tumor from a primary renal cortical neoplasm.