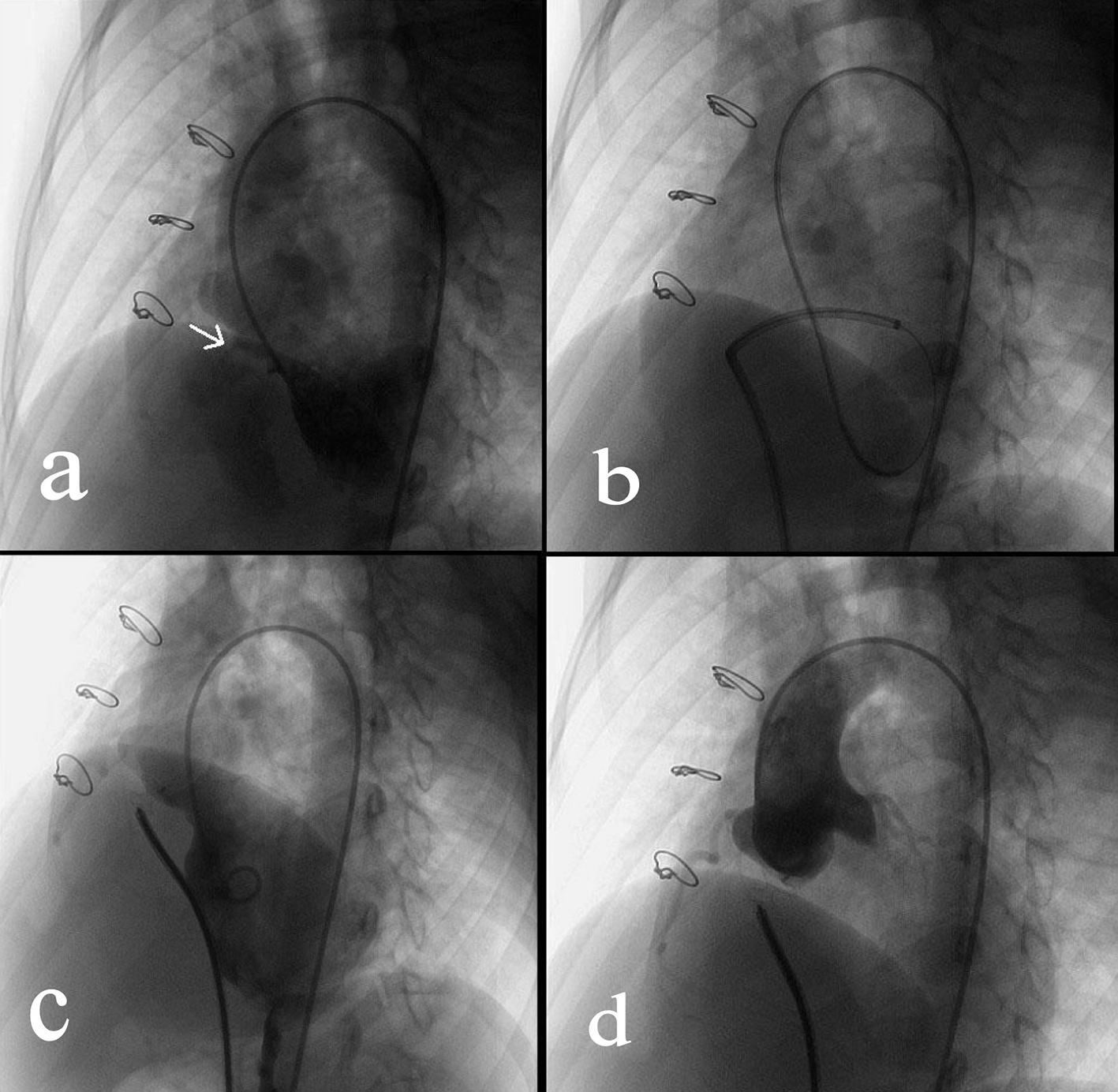
Figure 1. Transcatheter closure of a residual VSD. (a) Angiography of left ventricle via a 4F pigtail catheter inserted through the right femoral artery showed the residual VSD (indicated by the arrow). (b) Via the right femoral vein, a femoral vein-inferior vena cava-right ventricle-residual VSD-left ventricle-aorta-right femoral artery loop was established using a 260 cm loach guide wire. Afterwards, a 6-F delivery catheter was advanced along the loop to the left ventricle. (c) The loop wire was withdrawn. Subsequently, a VSD occluder was delivered to left ventricle and then opened in following sequence: left disc, waist and right disc. (d) After repeated angiography showed that the shunt disappeared, and then the occluder was released.
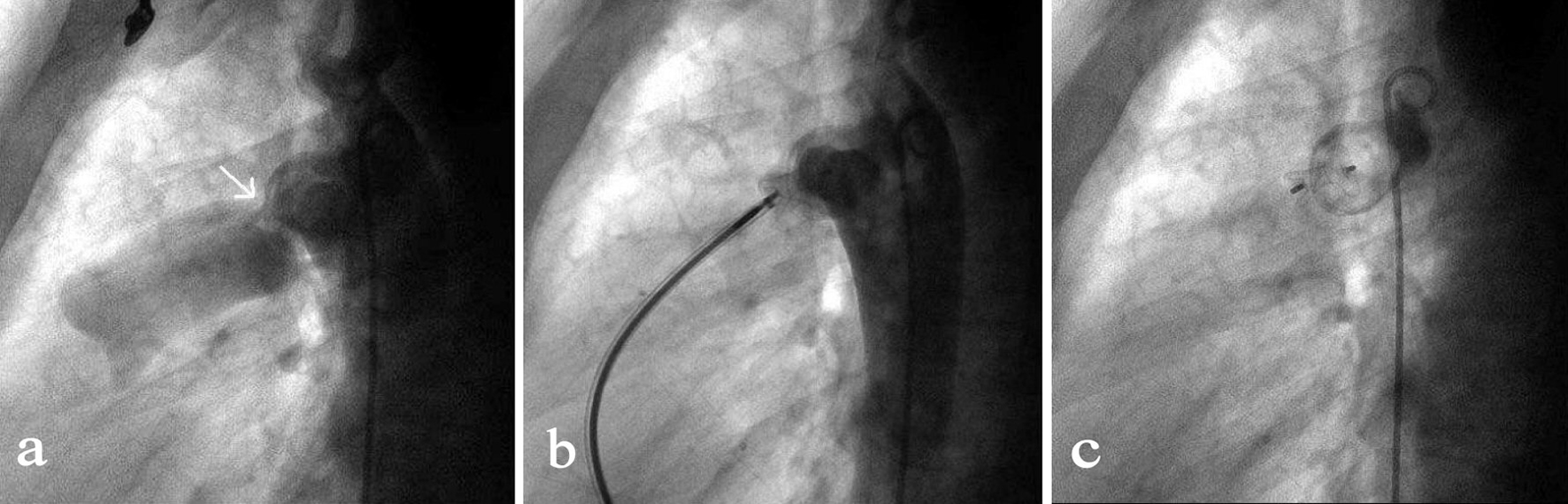
Figure 2. Transcatheter closure of a residual PDA. (a) Angiography of the aortic arch via a 5-F pigtail catheter that was inserted through the right femoral artery showed the residual PDA shunt (indicated by the arrow). (b) By the access of right femoral vein, a MPA2 catheter was advanced via right ventricle, pulmonary artery, PDA to the descending aorta followed by the insert of a 260 mm wire. After the MPA2 catheter was withdrawn, an 8-F delivery sheath was advanced along the wire and the duct occluder was delivered, positioned and opened in such a sequence that the aortic end of the occluder was first opened and then the pulmonary artery end. (c) Repeated angiography showed the occluder was properly placed and the shunt disappeared, and then the duct occluder was released.
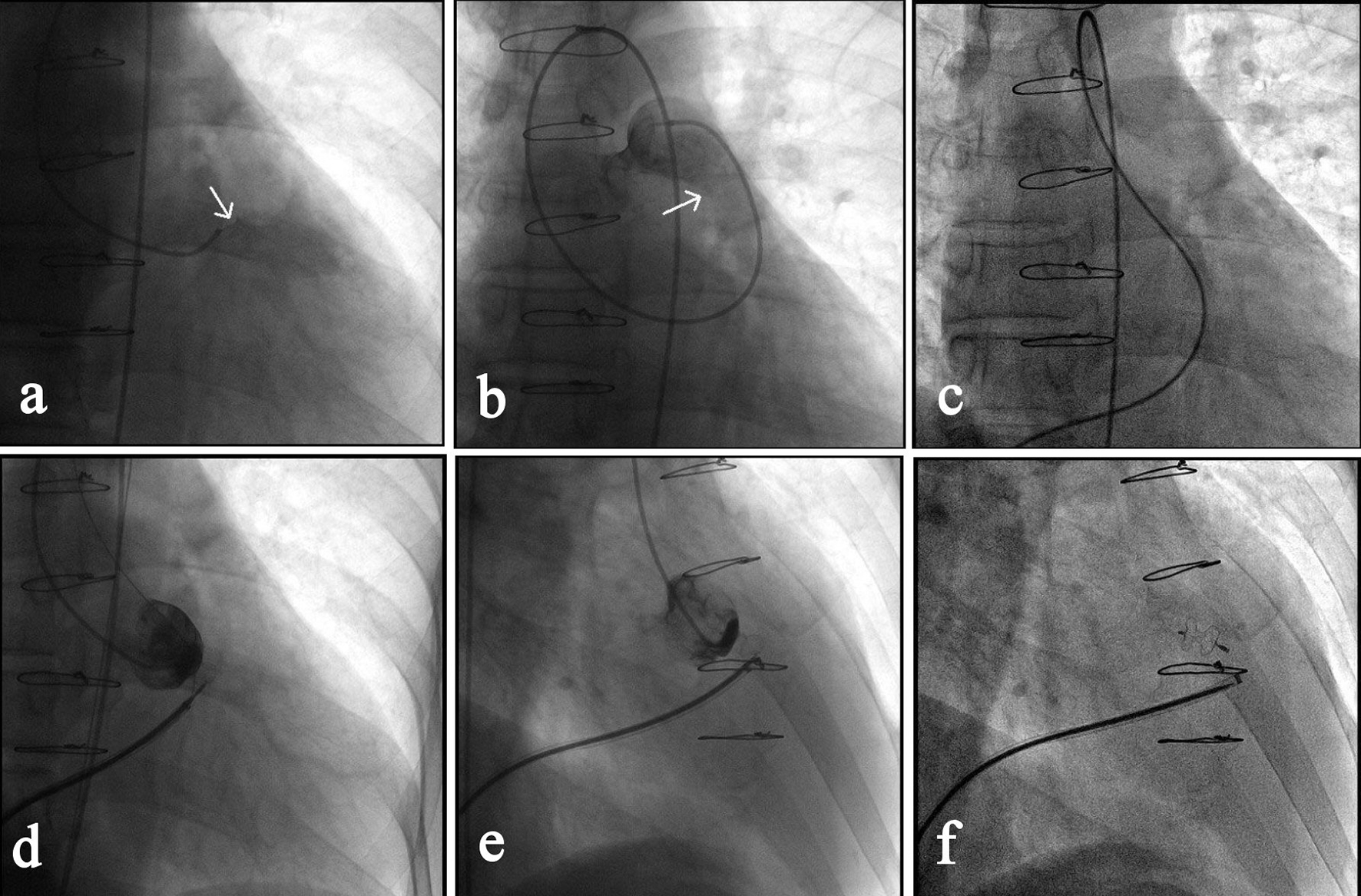
Figure 3. Transcatheter closure of a RSVA. (a) Angiography of right coronary sinus via a MPA1 catheter that was inserted into the right femoral artery showed the shunt from right coronary sinus to the right ventricular outflow tract (as indicated by the arrow). (b) Angiography after the MPA1 catheter was further advanced to the pulmonary artery confirmed the shunt (arrow). (c) Via the right femoral vein, a femoral vein-inferior vena cava-right ventricle-RSVA-aorta-right femoral artery loop was established using a 260 cm loach guide wire. (d) A 7-F delivery sheath was advanced along the loop to ascending aorta, and then a 7 mm VSD occluder was delivered passing the RSVA and opened in following sequence: left disc, waist and right disc. (e) The loop wire was withdrawn and angiography showed the shunt disappeared. (f) The occluder was released, delivery catheter withdrawn and repeated angiography showed the occluder was properly placed.