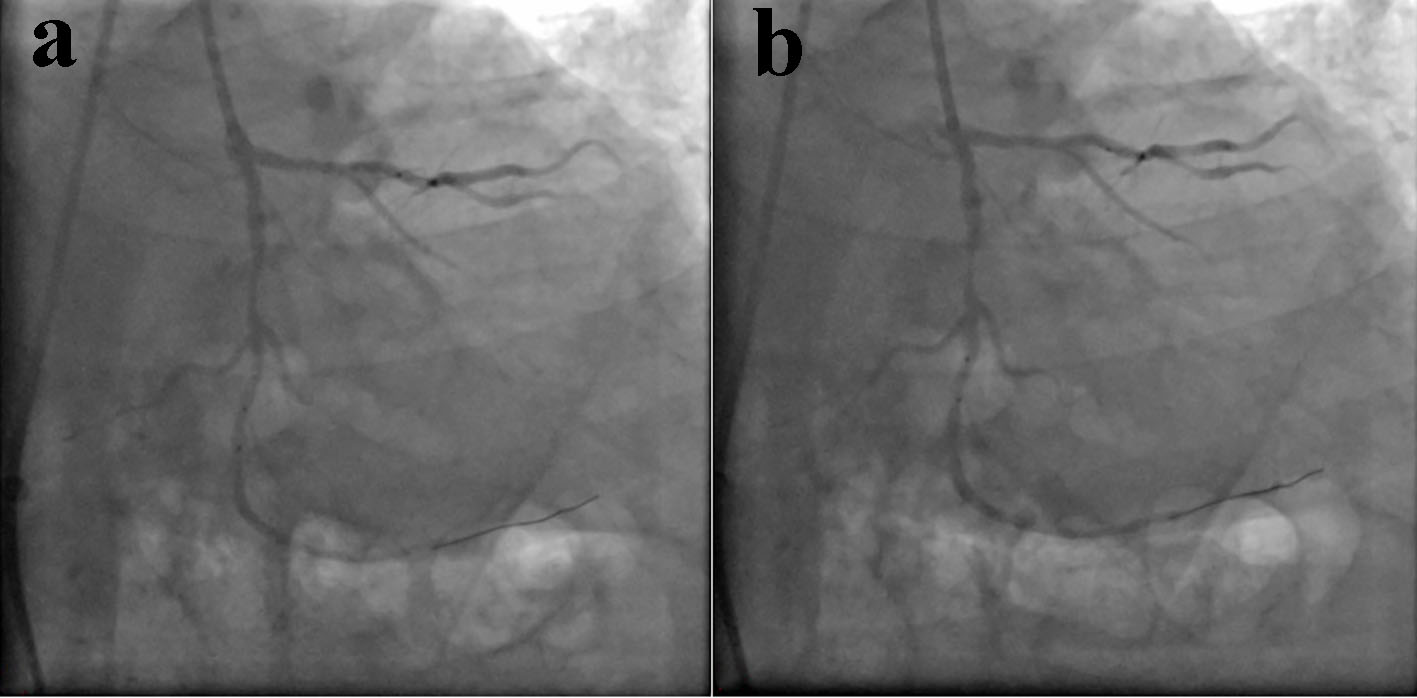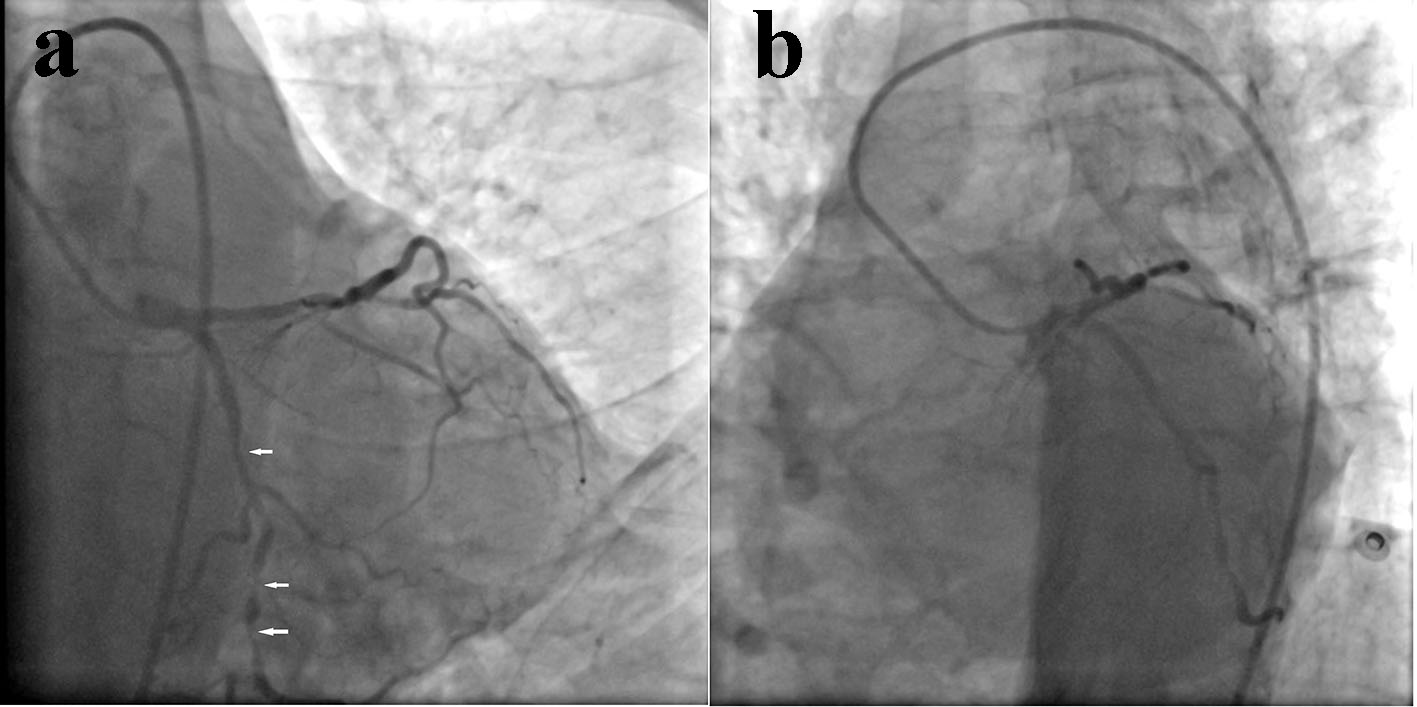
Figure 1. Angiogram showing diffuse, tortuous, calcified narrowing (90% stenosis) in left circumflex (LCx) coronary artery (a: AP caudal view; b: LAO caudal view).
| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Case Report
Volume 9, Number 1, February 2018, pages 63-67
Acute Stent Loss and Its Retrieval of a Long, Tapering Morph Stent in a Tortuous, Calcified Lesion
Figures