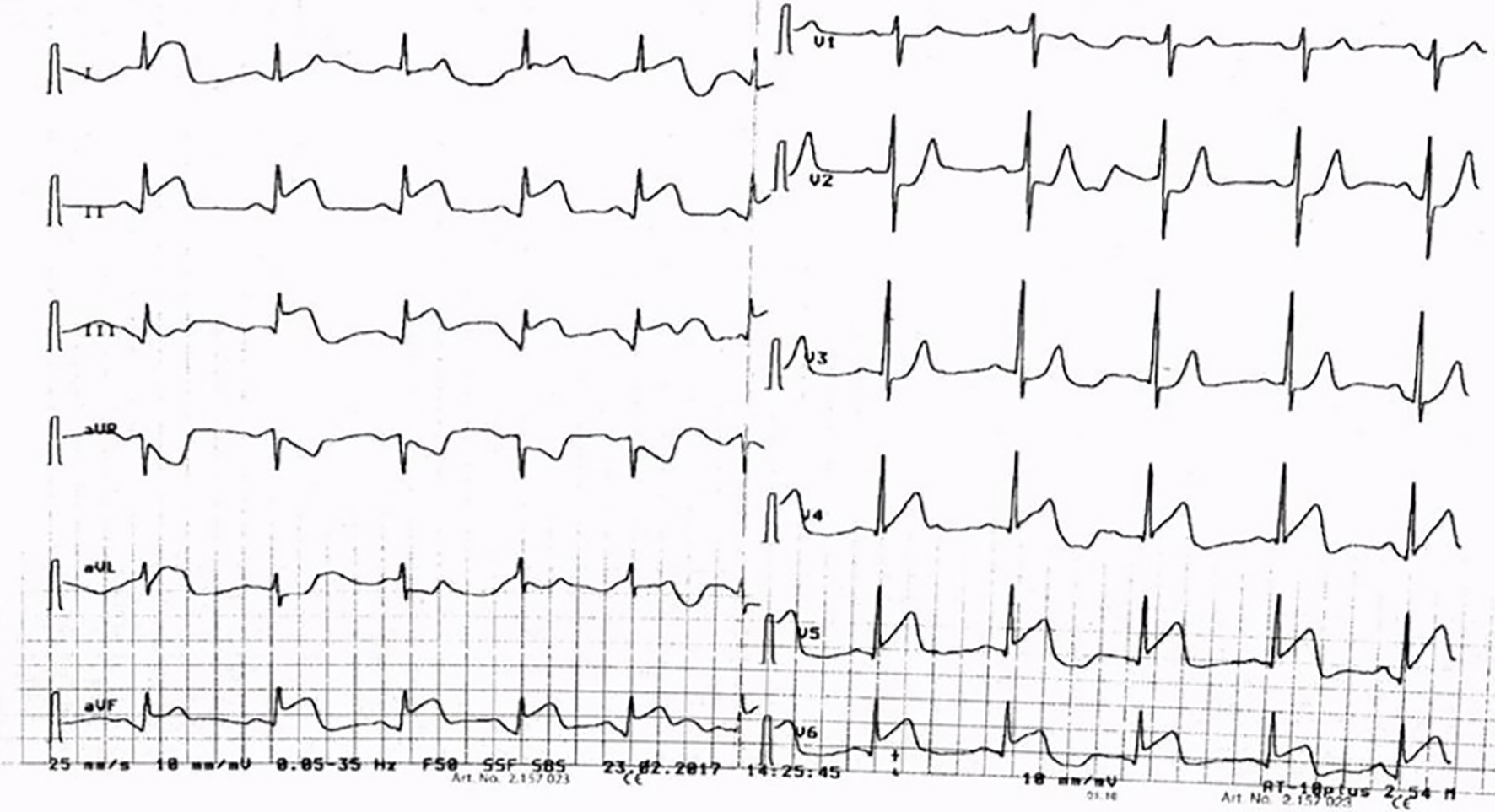
Figure 1. ECG showing STE in infero-lateral leads. ECG: electrocardiogram; STE: ST elevation.
| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Case Report
Volume 8, Number 6, December 2017, pages 331-335
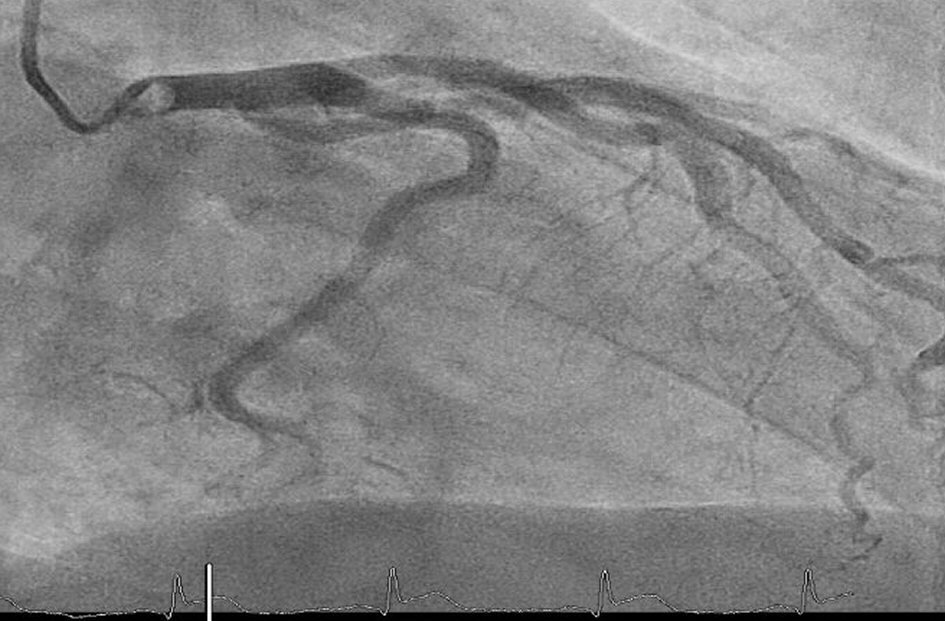
STEMI Due to Big Ostial Left Main Thrombus Extending Into Aorta: Challenging Situation With No Clear Guidelines
Figures


Table
| Test | Results |
|---|---|
| CK: creatine kinase; NT: N-terminal; BNP: brain natriuretic peptide. | |
| CK total (< 190 U/L) | 920 U/L |
| Myoglobin (28 - 72 µg/L) | 600 µg/L |
| Troponin T high sensitivity (< 14 ng/L) | 911 ng/L |
| NT-proBNP (< 85.8 ng/L) | 18 ng/L |
| Creatinine (44 - 80 µmol/L) | 66 µmol/L |