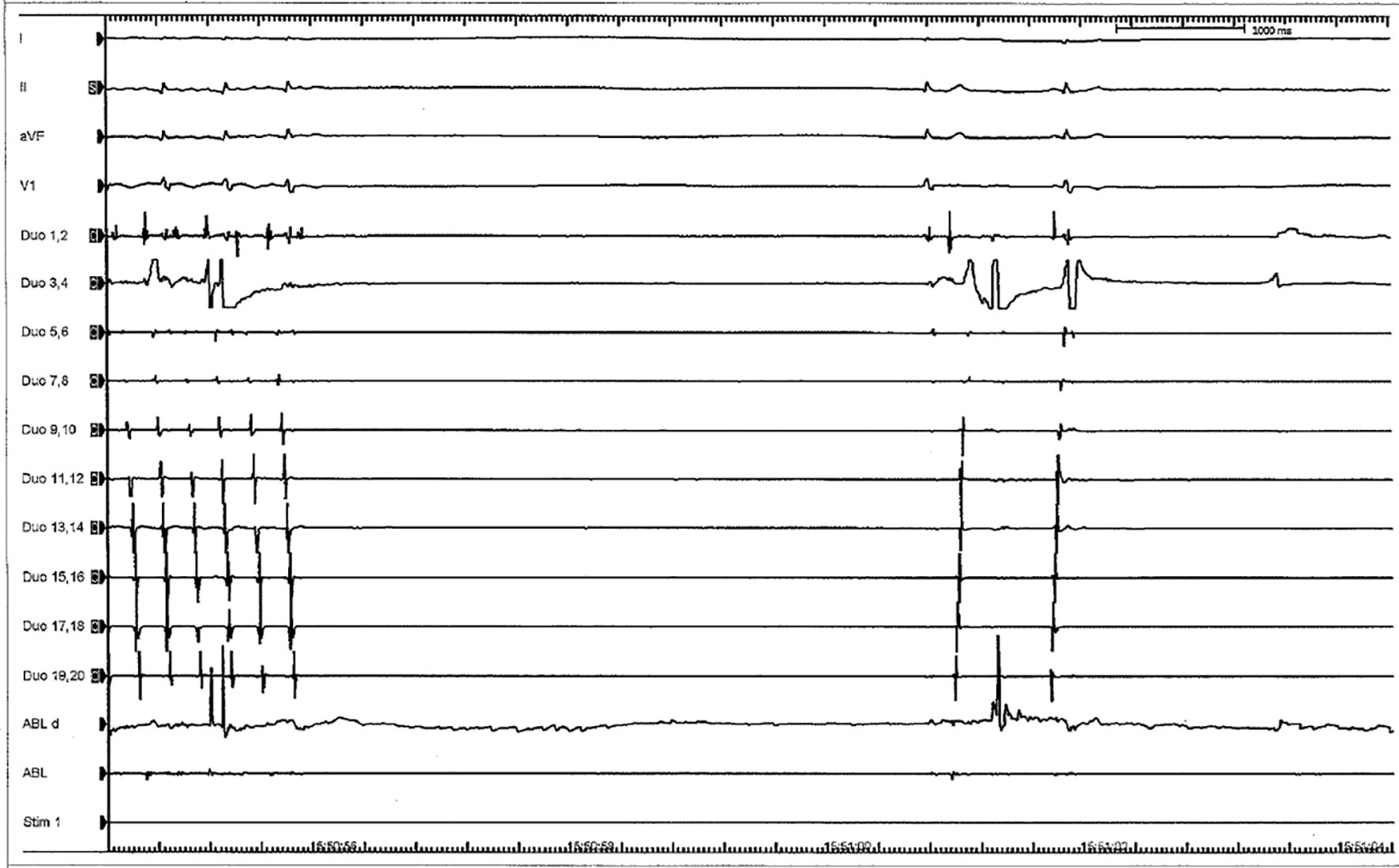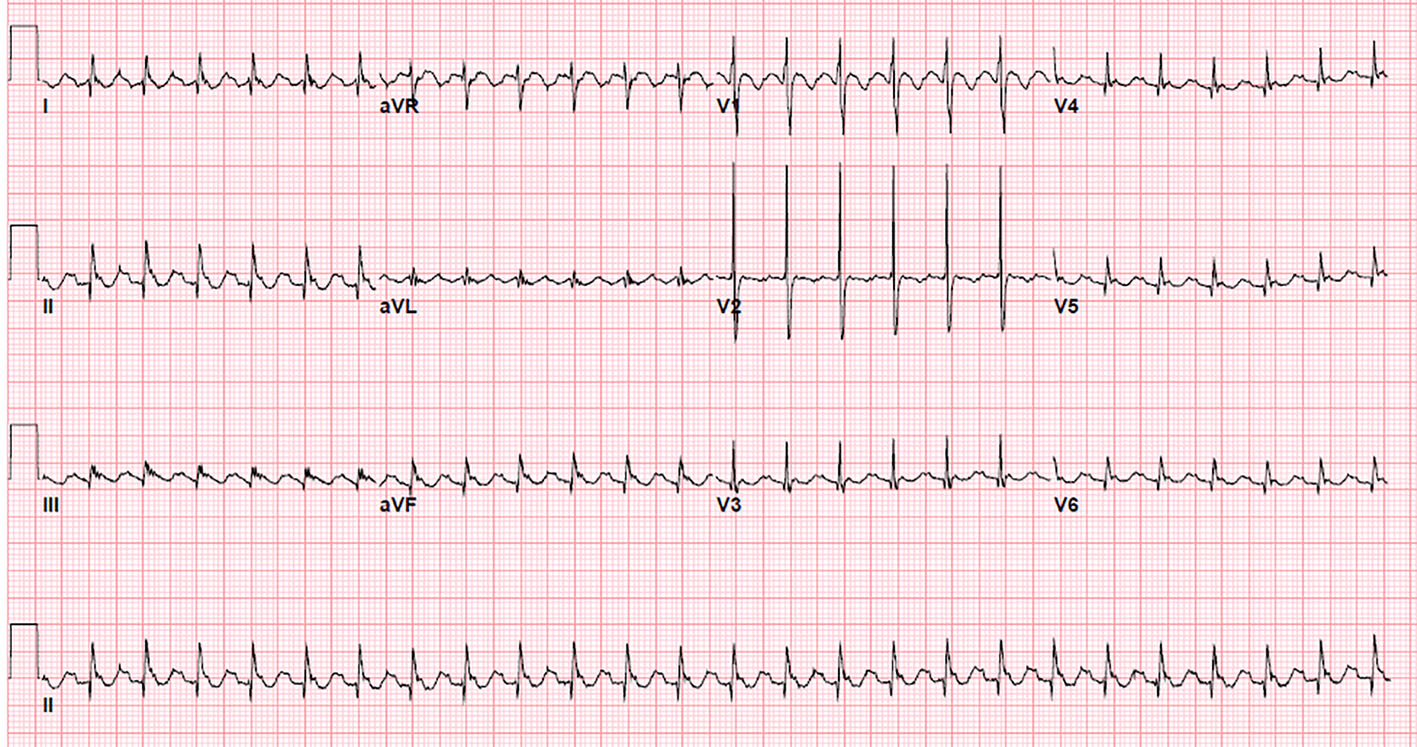
Figure 1. 12-lead surface electrogram showing saw tooth flutter waves: negative P waves in inferior leads and positive P waves in lead V1 and V2, suggestive of cavo-tricuspid isthmus dependent atrial flutter.
| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Case Report
Volume 8, Number 2, April 2017, pages 63-67
Cardiogenic Shock, Acute Severe Mitral Regurgitation and Complete Heart Block After Cavo-Tricuspid Isthmus Atrial Flutter Ablation
Figures