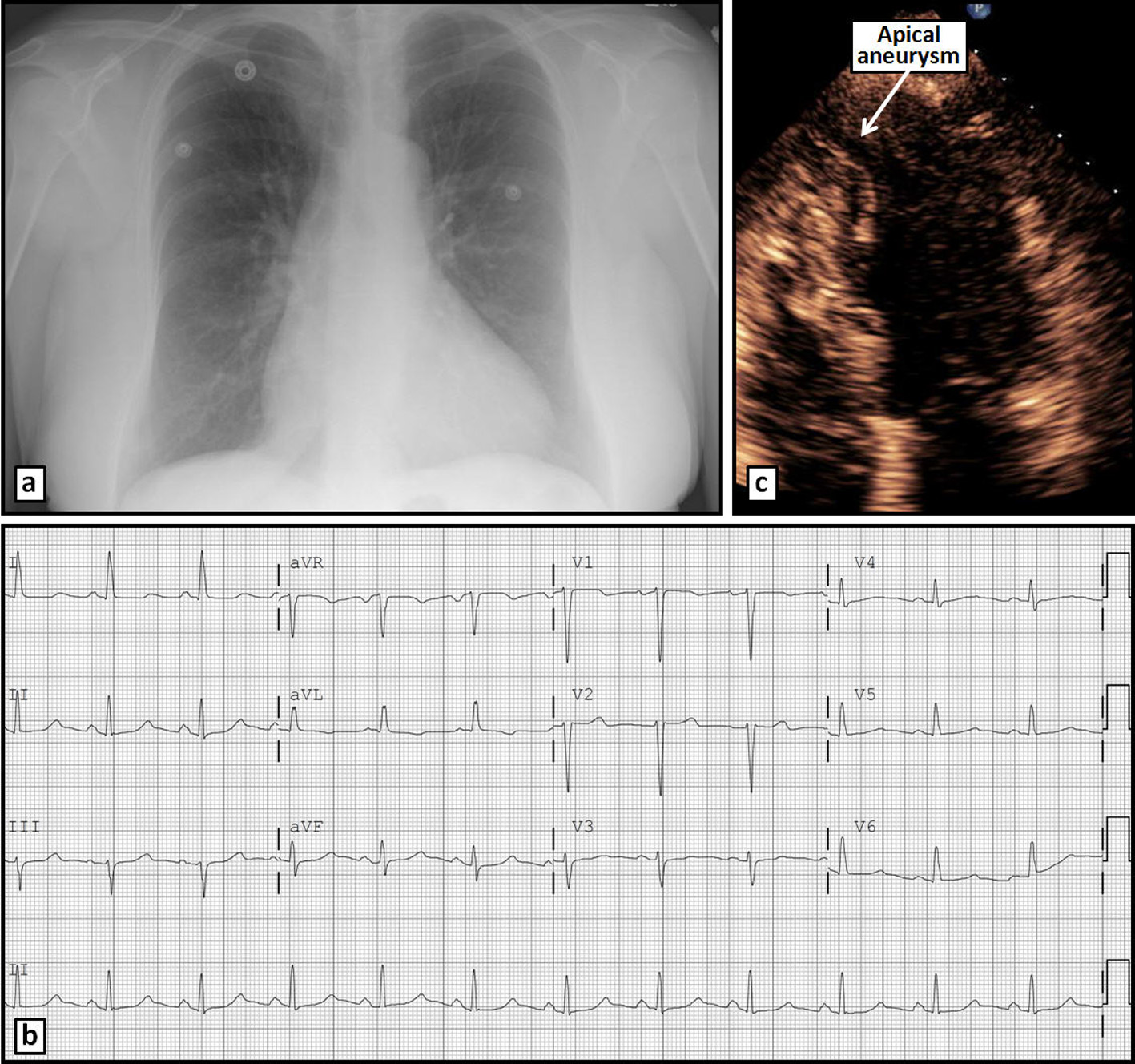
Figure 1. Chest radiograph (a) and ECG (b) on admission without significant abnormalities. Apical 4-chamber TTE view (c) reveals an apical aneurysm.
| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://www.cardiologyres.org |
Case Report
Volume 6, Number 6, December 2015, pages 352-356
Chest Pain With Apical Diverticulum in the Absence of Coronary Disease: Case Report and Review of the Literature
Figures
Table
| Characteristic | Fibrous | Muscular |
|---|---|---|
| Age | Adults | Children |
| Race | Predominately African Americans | No predilection |
| Prevalence | Not common | More Frequent |
| Histopathology | Mostly fibrous | Mostly muscular |
| Wall motion | Non-contractile, paradoxical motion | Contractile, synchronous motion |
| Segments affected | LV apical or subvalvular | LV apical; rarely RV |
| Complications reported | Aortic or mitral regurgitation; systemic embolism. Rupture. Arrhythmia | Rare complications |
| Associated abnormalities | No midline or congenital cardiac defects | Frequent midline and congenital cardiac defects |
| Angiography findings | No volume change during cardiac cycle | Volume reduction in systole and increase in diastole |
| MDCT findings | No volume change during cardiac cycle; fibrous tissue on diverticulum wall | Synchronous contraction with LV; myocardial tissue on diverticulum wall |
| CMR findings | Thin, fibrous wall; no volume change during cardiac cycle; no necrosis or fibrous tissue on delayed enhancement | Thin, contractile wall; no necrosis or fibrous tissue on delayed enhancement images |