*Average article statistics from the last 12 months data
COVID-19 RESEARCH
The COVID-19 outbreak presents the unprecedented challenge for world public and medical practitioners and health care providers, the post COVID-19 condition (or long COVID) includes long term symptoms which may persist for months or years after SARS-CoV-2 infection. We will consider submissions related to all aspects of COVID-19 and Long COVID, and process the manuscripts in priority.
Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access
Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc
Journal website http://www.cardiologyres.org
Original Article
Volume 8, Number 3, June 2017, pages 105-110
Comparison of Clopidogrel With Prasugrel and Ticagrelor in Patients With Acute Coronary Syndrome: Clinical Outcomes From the National Cardiovascular Database ACTION Registry
Mohamed Khayataa, Joseph N. Gabrab, M. Farhan Nassera, George I. Litmana, c, Shyam Bhaktaa, c, Rupesh Rainaa, d
aDepartment of Internal Medicine, Akron General Health System, Akron, OH, USA bDepartment of Research, Akron General Health System, Akron, OH, USA cSection of Cardiology, Department of Internal Medicine, Northeast Ohio University College of Medicine, Rootstown, OH, USA dCorresponding Author: Rupesh Raina, Adult-Pediatric Kidney Disease/Hypertension, Department of Nephrology, Cleveland Clinic Akron General and Akron Children’s Hospital, Akron, OH, USA; Faculty Staff at Case Western Reserve University School of Medicine, Cleveland, OH, USA
Manuscript submitted May 31, 2017, accepted June 5, 2017 Short title: Clopidogrel, Prasugrel and Ticagrelor in ACS doi: https://doi.org/10.14740/cr560w
Background: We aimed to compare the clinical outcomes of clopidogrel, prasugrel, and ticagrelor in clinical practice using the National Cardiovascular Database ACTION Registry®. Treatment guidelines for patients with acute coronary syndrome (ACS) undergoing percutaneous coronary intervention recommend dual antiplatelet therapy (DAPT) for 12 months. Few clinical trials have compared the safety and efficacy of clopidogrel with that of newer antiplatelet therapies.
Methods: A retrospective study of patients hospitalized for ACS at Cleveland Clinic Akron General was conducted. Data elements included detailed medical history and clinical outcomes during hospital stay. The primary outcome was a composite of major clinical events (cardiogenic shock, atrial fibrillation, ventricular fibrillation, ventricular tachycardia, heart failure, bleeding, and mechanical ventilation). The independent variable was the type of DAPT. Statistical analyses were performed using Chi-square and Mann-Whitney U tests. A post-hoc analysis was performed to compare between the antiplatelet drugs head-to-head.
Results: Subjects (n = 1,388) admitted between January 2011 and March 2016 with ACS and treated with clopidogrel, prasugrel, or ticagrelor were included in the study. Mean age was 65 ± 14 years and 46% had ST-segment elevation myocardial infarction. Prasugrel administration within 24 h was associated with a lower incidence of the composite outcome (P = 0.049), bleeding (P = 0.028), and heart failure (P = 0.002).
Conclusion: There was a significant difference between the type of antiplatelet drug and clinical outcomes in ACS patients who were treated with DAPT. Observations from current study may provide important information for prescribers in clinical decision-making.
Keywords: Antiplatelet therapy; Coronary artery disease; Health care outcomes
About 1.1 million people in the United States are diagnosed every year with acute coronary syndrome (ACS) [1]. Despite advances in prevention, diagnosis, and management, myocardial infarction remains a common cause of death, disability, poor quality of life, and preventable health-care expenditure worldwide [2]. There has been a search for the ideal antiplatelet agent to accompany aspirin as part of dual antiplatelet treatment in patients with ACS with and without ST-segment elevation myocardial infarction (STEMI) [3].
Current treatment guidelines for patients with ACS undergoing percutaneous coronary intervention (PCI) recommend dual antiplatelet therapy (DAPT), a combination of aspirin and a P2Y12 inhibitor, for at least 12 months after the ACS event [3-6]. DAPT is crucial to prevent major adverse events, such as cardiovascular death, myocardial infarction (MI), stroke, and stent thrombosis in patients with ACS [7]. Clopidogrel remains the P2Y12 inhibitor used most widely; however, incremental benefits compared with clopidogrel have been shown with the more potent P2Y12 inhibitors, e.g. prasugrel and ticagrelor [8, 9].
In contrast to clopidogrel, ticagrelor and prasugrel have faster onset of action and have less inter-individual variation with respect to drug effects [10-12]. Ticagrelor has another advantage in that it is direct acting and reversible [13]. Advantages of ticagrelor and prasugrel make them more suitable for the treatment of patients with a high thrombotic risk. However, the matter gets complicated when patients have both a high thrombotic and bleeding risk [9, 11] in which cases prescribers tend to pick the safest drug. Prasugrel was proven in recent clinical trials to be more efficacious than clopidogrel, with reduced ischemic events, but with increased major bleeding, including fatal bleeding [9, 11]. In a large phase 3 trial of ACS patients with or without STEMI, ticagrelor reduced death from vascular causes, MI, or stroke compared to clopidogrel [11]. In addition, there was no difference in major bleeding events between the two groups, but there was an increase in non-procedure related bleeding events in patients receiving ticagrelor [11].
Guidelines of the American Heart Association/American College of Cardiology and the European Society of Cardiology recommend ticagrelor or prasugrel over clopidogrel for patients with ACS undergoing PCI who can take these drugs safely [3, 5, 6, 14]. Both prasugrel and ticagrelor have been assigned a class 1B recommendation for patients with ACS, especially for those undergoing PCI [15].
There have been few studies comparing the safety and efficacy of clopidogrel with that of prasugrel and ticagrelor [7, 9, 11, 16]. We aim to compare between the type of antiplatelet drug (clopidogrel, prasugrel, or ticagrelor) and the clinical outcomes during hospital stay in a clinical practice using a single-center registry through the National Cardiovascular Database ACTION Registry®. We also performed a head-to-head comparison between antiplatelet drugs using post-hoc analysis.
A retrospective cohort study of patients hospitalized for ACS and prescribed aspirin plus either clopidogrel, prasugrel, or ticagrelor was conducted using the ACTION Registry® at Cleveland Clinic Akron General. Data elements included all inpatient encounters within the facility, with detailed medical history, medications, and clinical outcomes during hospital stay. Informed consent was waived, as this was a chart review study with de-identified patient data. The study was approved by the local Institutional Review Board.
Adult patients (aged ≥ 18 years of age) who had an index hospital admission and discharge between January 2011 and March 2016, with the diagnosis of ACS were identified. Patients who were treated with aspirin and clopidogrel, prasugrel, or ticagrelor within 24 h of admission were included in the analyses.
Baseline information included demographic data, and comorbidities (hypertension, smoking status, heart failure, dyslipidemia, diabetes mellitus, history of MI, atrial fibrillation, atrial flutter, prior PCI, prior coronary bypass surgery, cerebrovascular disease, stroke or transient ischemic attack, peripheral vascular disease, and dialysis-dependent end-stage renal disease) were identified via diagnosis-related data from hospitalization records. The type of ACS was classified based on electrocardiogram (EKG) findings (ST-segment elevation, new or presumed new left bundle branch, ST-segment depression or T-wave changes, or no EKG changes).
The primary outcome was a composite of major adverse clinical events within the hospital consisting of the patient having at least one of the following: cardiogenic shock, atrial fibrillation, ventricular fibrillation, ventricular tachycardia, heart failure, bleeding, and mechanical ventilation. Bleeding included retroperitoneal, gastrointestinal, and genitourinary bleeding. Each individual clinical event was included in separate analyses as secondary outcomes.
Statistical analysis
Chi-square, for categorical variables, and Mann-Whitney U tests, for continuous variables, were used to determine if the composite clinical event was dependent on baseline characteristics (e.g. demographics, comorbidities, medication use, EKG findings, etc.). In addition, Chi-square tests (2 × 3) were used to determine if the composite and individual clinical events were dependent on antiplatelet type (clopidogrel, prasugrel, and ticagrelor); post-hoc analyses were performed using standardized (adjusted) Pearson’s residuals with a Bonferroni correction. Where appropriate, Fisher’s exact tests and Yate’s Chi-squared tests were used. In addition, odds ratios (ORs) with 95% confidence intervals (CIs) were also calculated. A significance level of 0.05 was used for all statistical analyses.
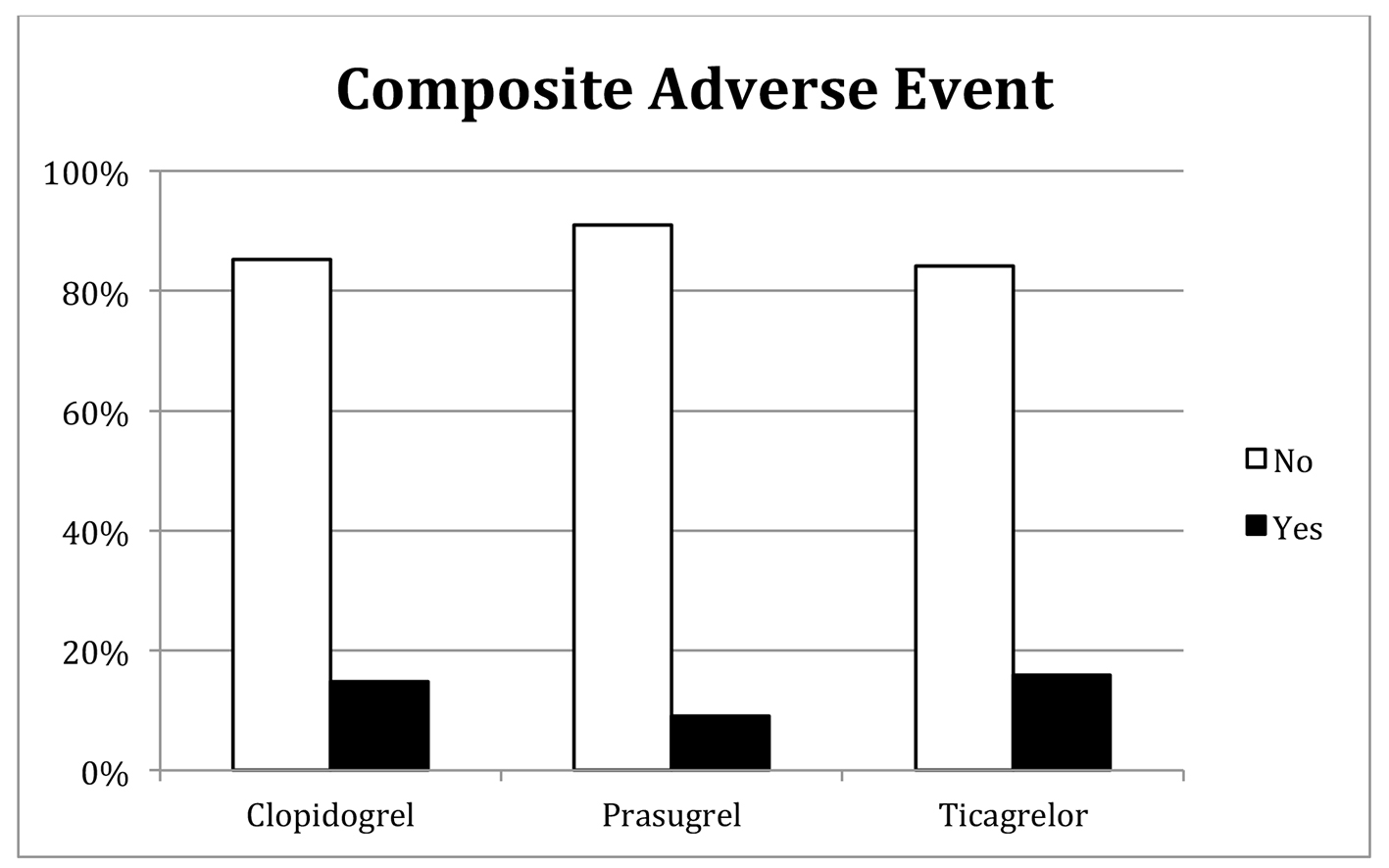
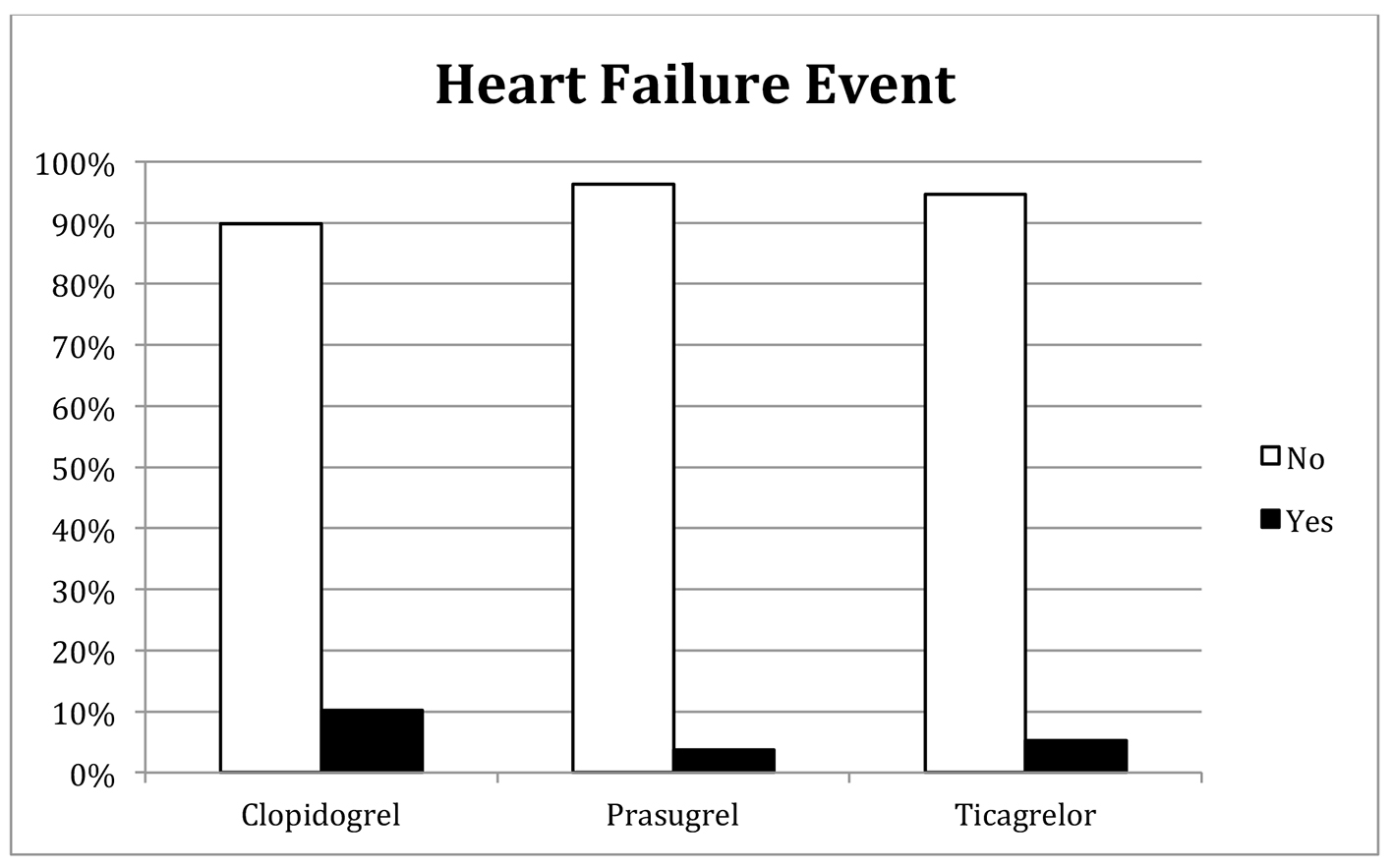
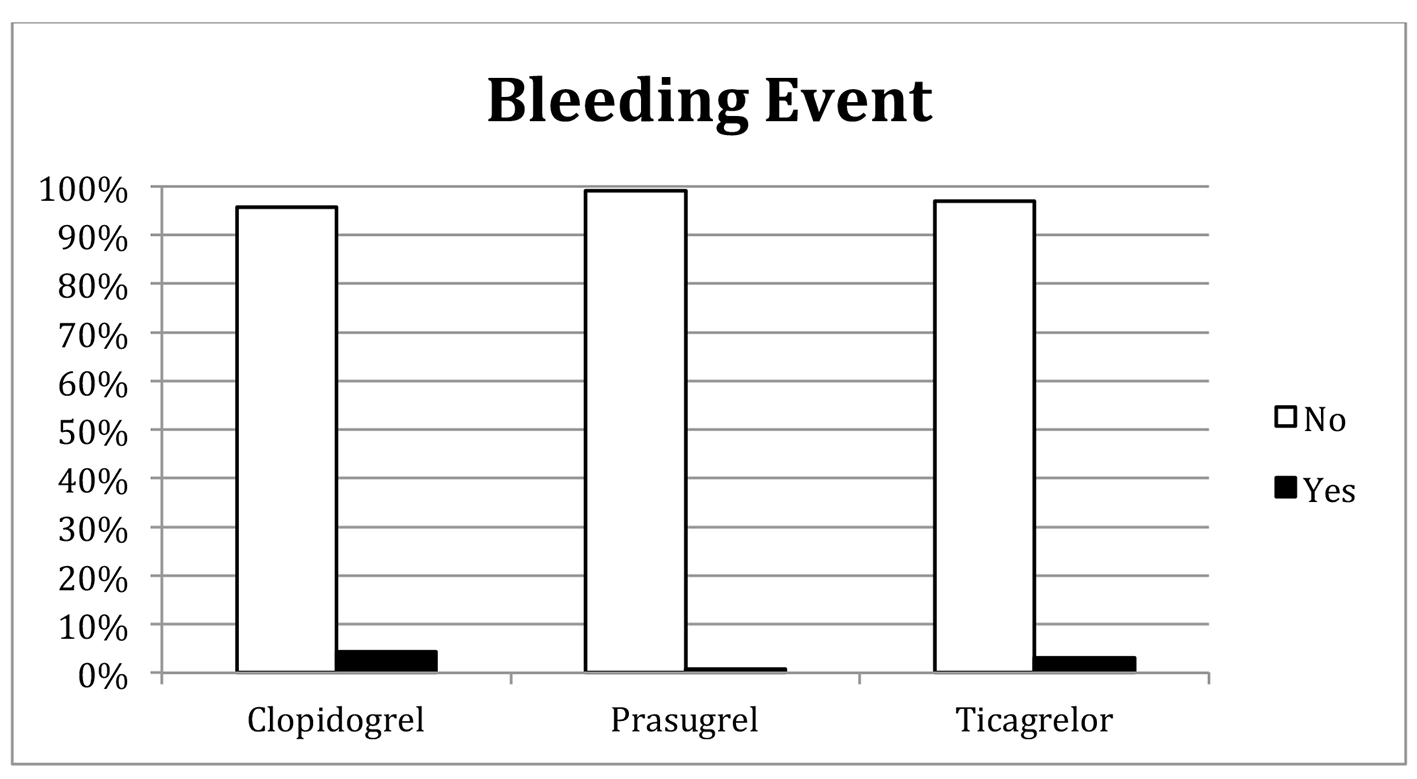
We identified 1,388 adult patients hospitalized and discharged with the diagnosis of ACS and were treated with aspirin and an oral antiplatelet medication (clopidogrel, prasugrel, or ticagrelor) within 24 h of admission. A total of 1,012 patients received clopidogrel, 244 patients received prasugrel, and 132 patients received ticagrelor. Fourteen percent of total patients had the incidence of composite clinical outcome, 1% developed atrial fibrillation, 1.2% developed ventricular fibrillation or ventricular tachycardia, 0.4% placed on mechanical ventilation support, 5% developed cardiogenic shock, 8.6% developed heart failure, and 3.6% developed bleeding.
Key patient baseline demographic and clinical characteristics are summarized in Table 1.
Table 1. Association Between Baseline Characteristics and Composite Clinical Outcome
When antiplatelet drugs were compared head-to-head, there was a significant association between the type of antiplatelet and the incidence of the composite cardiac outcome (P = 0.049), heart failure (P = 0.002), and bleeding (P = 0.028). Specifically, patients who received prasugrel had a lower incidence than expected for the composite cardiac outcome, heart failure, and bleeding; patients who were administered clopidogrel had a higher incidence of heart failure and bleeding than expected (Table 2, Figs. 1-3).
This study compares the safety between the three antiplatelet drugs (i.e. clopidogrel, prasugrel, and ticagrelor) combined with aspirin during hospital stay as they are used in clinical practice. Decisions regarding use of the new antiplatelet drugs are influenced mainly by safety considerations [16-18]. Cost of extended hospital stay due to complications must be taken into account as well.
This study demonstrated that patients treated with prasugrel within 24 h of admission had lower incidence of the clinical composite adverse event, heart failure, and bleeding compared to those treated with clopidogrel and ticagrelor. The presented findings are partly supported by TRITON-TIMI 38 trial, one of the first clinical trials that compared between prasugrel and clopidogrel in ACS patients [12]. The TRITON-TIMI 38 trial showed that both loading and maintenance dose of prasugrel has higher efficacy than clopidogrel [12].
The TRITON-TIMI 38 trial also demonstrated that ACS patients treated with prasugrel had a higher incidence of bleeding on long-term follow-up [12, 19]. However, those reported findings conflict with other studies. For example, previous studies concluded that there was no difference in bleeding incidence between prasugrel and clopidogrel [20, 21]. Other studies demonstrated that prasugrel, compared to clopidogrel, had more frequent minor/minimal bleeding events but fewer incidences of major bleeding events [22, 23]. The findings of the presented study determined that patients receiving prasugrel had a lower incidence of in-hospital major bleeding events compared to those administered clopidogrel, agreeing with the latter previous studies with long-term follow-up [22, 23]. The lower incidence of major bleeding among the prasugrel group may be explained by selection bias such that prasugrel is prescribed to patients with a low risk of bleeding [22, 24].
Patients, with ACS, administered prasugrel also had a lower incidence of heart failure than those that were administered clopidogrel. The findings of the presented study agree with those at long-term follow-up for the INFUSE-AMI trial [20].
As with all observational researches, there are inherent limitations in the conclusions to be drawn from this single-center, non-randomized study as it can demonstrate only associations, not causality. A second limitation is that the number of patients who received ticagrelor within 24 h of admission is less than that who received clopidogrel and prasugrel. This difference may be explained, in part, by the fact that ticagrelor was approved more recently than the other antiplatelet agents, which had been commercially available for a longer duration. Future studies can be performed with more data-points for ticagrelor. A third limitation of our study is that it addressed only in-hospital clinical events, as there was no mandated follow-up of patients following discharge. Another limitation is that choice of antithrombotic agent (heparin or bivalirudin), heparin dose, and active clotting times achieved, were not available in our dataset. Finally, access site, provider experience, or access to drug due to insurance and formulary reasons, which may influence medication choice of medications, were not available for this patient population.
Conclusion
In this single-center, registry-based, and observational study, we found a significant association between the choice of antiplatelet therapy and in-hospital clinical outcomes in patients with ACS. When the three types of antiplatelet drugs compared head-to-head, prasugrel was the safest drug with lower incidences of heart failure and bleeding; higher incidences of heart failure and bleeding were found among patients who received clopidogrel. Our study may assist prescribers in clinical decision-making.
Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, de Ferranti S, et al. Heart disease and stroke statistics - 2015 update: a report from the American Heart Association. Circulation. 2015;131(4):e29-322. doipubmed
Cayla G, Silvain J, O’Connor SA, Collet JP, Montalescot G. Current antiplatelet options for NSTE-ACS patients. QJM. 2012;105(10):935-948. doipubmed
Hamm CW, Bassand JP, Agewall S, Bax J, Boersma E, Bueno H, Caso P, et al. ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: The Task Force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2011;32(23):2999-3054. doipubmed
Amsterdam EA, Wenger NK, Brindis RG, Casey DE, Jr., Ganiats TG, Holmes DR, Jr., Jaffe AS, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;130(25):e344-426. doipubmed
O’Gara PT, Kushner FG, Ascheim DD, Casey DE, Jr., Chung MK, de Lemos JA, Ettinger SM, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127(4):529-555. doipubmed
Task Force Members, Steg PG, James SK, Atar D, Badano LP, Blomstrom-Lundqvist C, Borger MA, et al. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology (ESC). Eur Heart J. 2012;33(20):2569-2619. doi
Qaderdan K, Ishak M, Heestermans AA, de Vrey E, Jukema JW, Voskuil M, de Boer MJ, et al. Ticagrelor or prasugrel versus clopidogrel in elderly patients with an acute coronary syndrome: Optimization of antiplatelet treatment in patients 70 years and older - rationale and design of the POPular AGE study. Am Heart J. 2015;170(5):981-985.e1. doipubmed
Cai C, Li YX, Xi HJ, Song BN, Han DM. [Anatomical study of auditory brainstem implantation through retrosigmoid approach]. Zhonghua Yi Xue Za Zhi. 2009;89(20):1395-1398. pubmed
Wiviott SD, Braunwald E, McCabe CH, Montalescot G, Ruzyllo W, Gottlieb S, Neumann FJ, et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2007;357(20):2001-2015. doipubmed
James S, Akerblom A, Cannon CP, Emanuelsson H, Husted S, Katus H, Skene A, et al. Comparison of ticagrelor, the first reversible oral P2Y(12) receptor antagonist, with clopidogrel in patients with acute coronary syndromes: Rationale, design, and baseline characteristics of the PLATelet inhibition and patient Outcomes (PLATO) trial. Am Heart J. 2009;157(4):599-605. doipubmed
Wallentin L, Becker RC, Budaj A, Cannon CP, Emanuelsson H, Held C, Horrow J, et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2009;361(11):1045-1057. doipubmed
Antman EM, Wiviott SD, Murphy SA, Voitk J, Hasin Y, Widimsky P, Chandna H, et al. Early and late benefits of prasugrel in patients with acute coronary syndromes undergoing percutaneous coronary intervention: a TRITON-TIMI 38 (Trial to assess improvement in therapeutic outcomes by optimizing platelet inhibition with prasugrel-thrombolysis in myocardial infarction) analysis. J Am Coll Cardiol. 2008;51(21):2028-2033. doipubmed
Wallentin L. P2Y(12) inhibitors: differences in properties and mechanisms of action and potential consequences for clinical use. Eur Heart J. 2009;30(16):1964-1977. doipubmed
Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, 3rd, Guyton RA, O’Gara PT, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(23):2440-2492. doipubmed
Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, Chambers CE, et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation. 2011;124(23):e574-651. doipubmed
Chatterjee S, Ghose A, Sharma A, Guha G, Mukherjee D, Frankel R. Comparing newer oral anti-platelets prasugrel and ticagrelor in reduction of ischemic events-evidence from a network meta-analysis. J Thromb Thrombolysis. 2013;36(3):223-232. doipubmed
Biondi-Zoccai G, Lotrionte M, Agostoni P, Abbate A, Romagnoli E, Sangiorgi G, Angiolillo DJ, et al. Adjusted indirect comparison meta-analysis of prasugrel versus ticagrelor for patients with acute coronary syndromes. Int J Cardiol. 2011;150(3):325-331. doipubmed
Steiner S, Moertl D, Chen L, Coyle D, Wells GA. Network meta-analysis of prasugrel, ticagrelor, high- and standard-dose clopidogrel in patients scheduled for percutaneous coronary interventions. Thromb Haemost. 2012;108(2):318-327. doipubmed
Zeymer U, Hochadel M, Lauer B, Kaul N, Wohrle J, Andresen D, Schwimmbeck P, et al. Use, efficacy and safety of prasugrel in patients with ST segment elevation myocardial infarction scheduled for primary percutaneous coronary intervention in clinical practice. Results of the prospective ATACS-registry. Int J Cardiol. 2015;184:122-127. doipubmed
Brener SJ, Oldroyd KG, Maehara A, El-Omar M, Witzenbichler B, Xu K, Mehran R, et al. Outcomes in patients with ST-segment elevation acute myocardial infarction treated with clopidogrel versus prasugrel (from the INFUSE-AMI trial). Am J Cardiol. 2014;113(9):1457-1460. doipubmed
Montalescot G, Wiviott SD, Braunwald E, Murphy SA, Gibson CM, McCabe CH, Antman EM, et al. Prasugrel compared with clopidogrel in patients undergoing percutaneous coronary intervention for ST-elevation myocardial infarction (TRITON-TIMI 38): double-blind, randomised controlled trial. Lancet. 2009;373(9665):723-731. doi
Bacquelin R, Oger E, Filippi E, Hacot JP, Auffret V, Le Guellec M, Coudert I, et al. Safety of prasugrel in real-world patients with ST-segment elevation myocardial infarction: 1-year results from a prospective observational study (Bleeding and Myocardial Infarction Study). Arch Cardiovasc Dis. 2016;109(1):31-38. doipubmed
Lattuca B, Fabbro-Peray P, Leclercq F, Schmutz L, Ledermann B, Cornillet L, Benezet JF, et al. One-year incidence and clinical impact of bleeding events in patients treated with prasugrel or clopidogrel after ST-segment elevation myocardial infarction. Arch Cardiovasc Dis. 2016;109(5):337-347. doipubmed
Almendro-Delia M, Blanco Ponce E, Gomez-Dominguez R, Gonzalez-Matos C, Lobo-Gonzalez M, Caballero-Garcia A, Hidalgo-Urbano R, et al. Safety and efficacy of in-hospital clopidogrel-to-prasugrel switching in patients with acute coronary syndrome. An analysis from the ‘real world’. J Thromb Thrombolysis. 2015;39(4):499-507. doipubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.